

Cardiac function, haemodynamics, and valve competence with exercise in patients with heart failure with preserved ejection fraction and mild to moderate secondary mitral regurgitation
- PMID: 38837599
- PMCID: PMC11356312
- DOI: 10.1002/ejhf.3322
Cardiac function, haemodynamics, and valve competence with exercise in patients with heart failure with preserved ejection fraction and mild to moderate secondary mitral regurgitation
Abstract
Aims: This study aimed to evaluate the clinical significance of secondary mitral regurgitation (MR) in patients with heart failure with preserved ejection fraction (HFpEF).
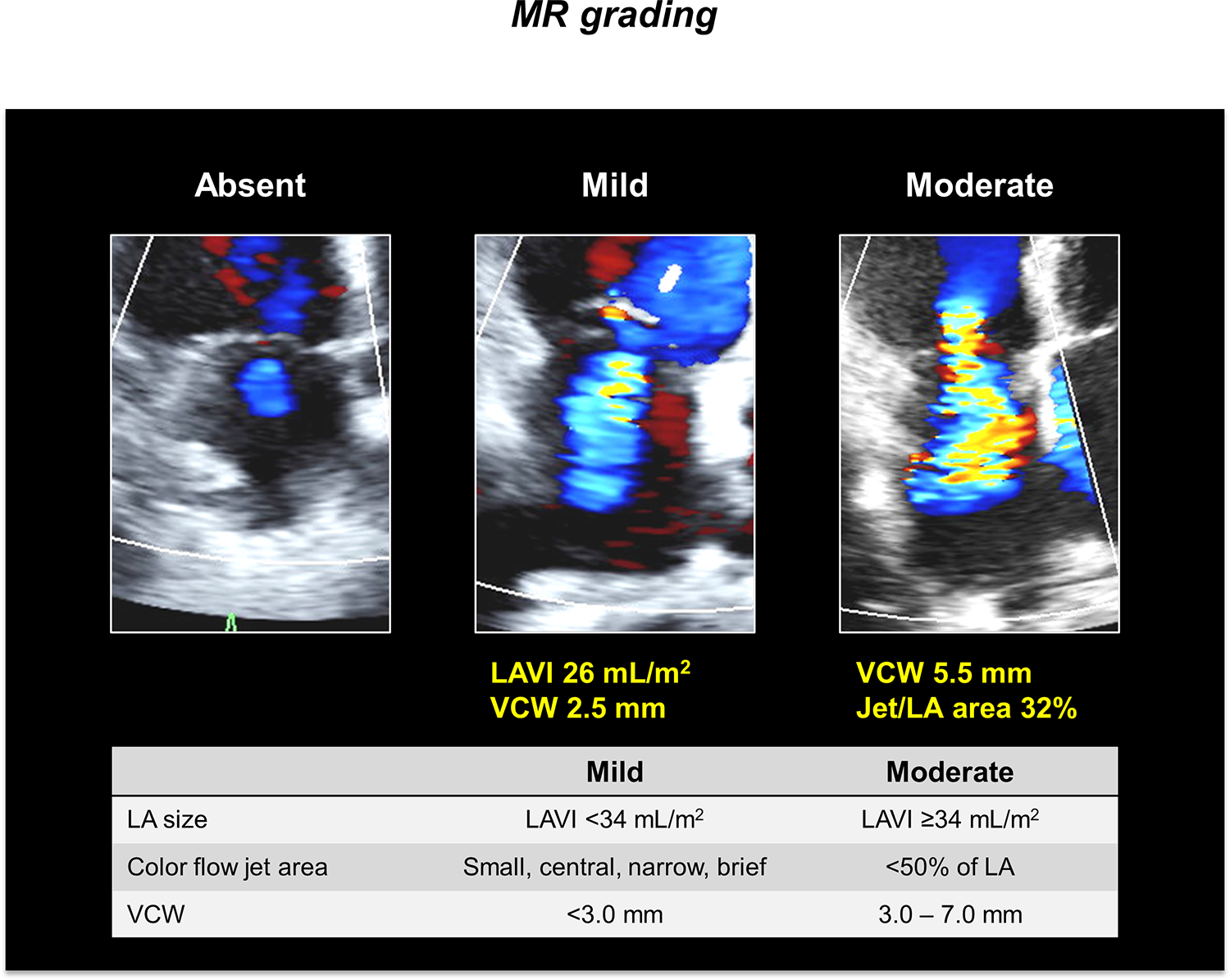
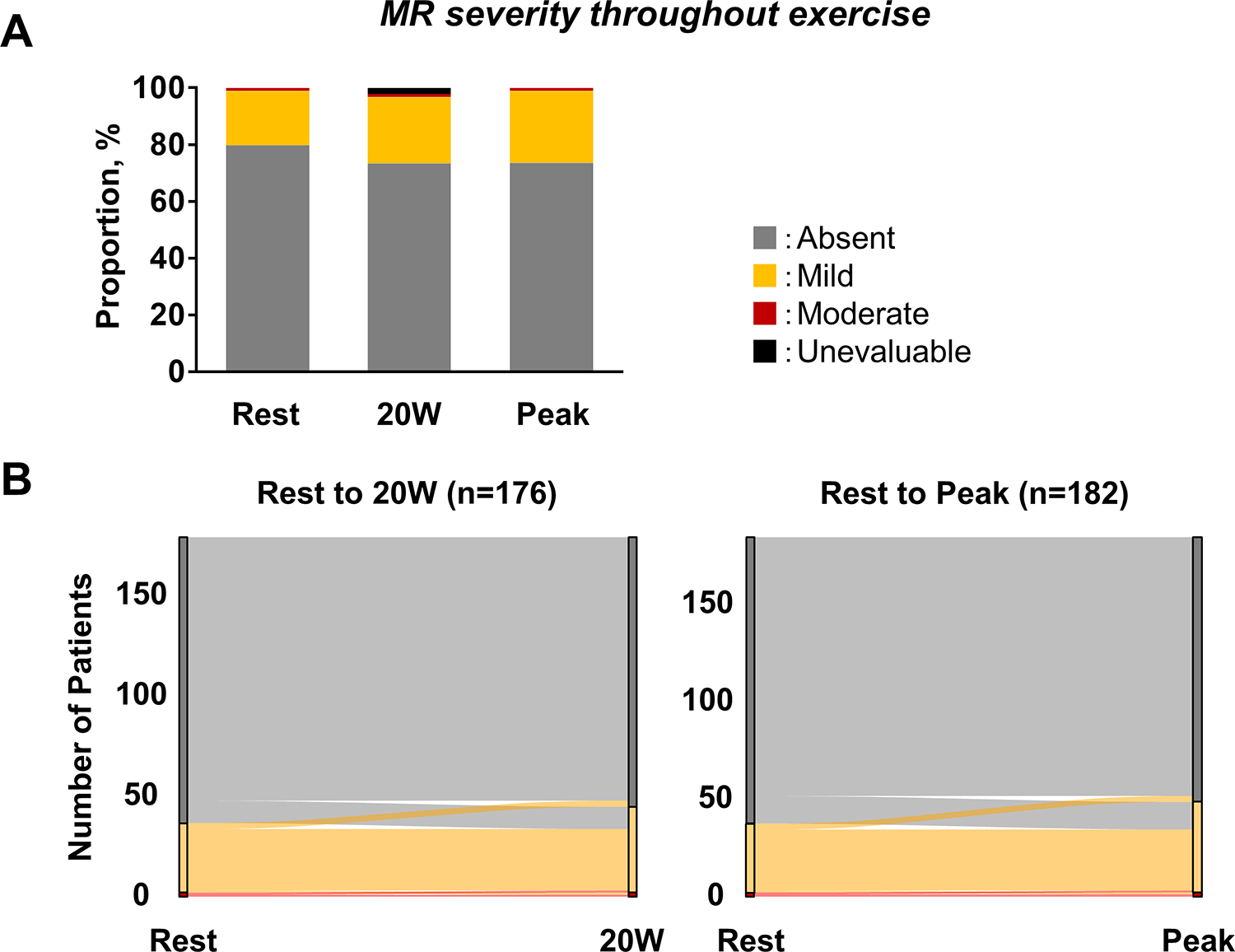
Methods and results: We conducted a prospective study enrolling consecutively evaluated patients with HFpEF undergoing invasive haemodynamic exercise testing with simultaneous echocardiography. Compared to HFpEF without MR (n = 145, 79.7%), those with mild or moderate MR (n = 37, 20.3%) were older, more likely to be women, had more left ventricular (LV) systolic dysfunction, and more likely to have left atrial (LA) myopathy reflected by greater burden of atrial fibrillation, more LA dilatation, and poorer LA function. Pulmonary artery (PA) wedge pressure was higher at rest in HFpEF with MR (17 ± 5 mmHg vs. 20 ± 5 mmHg, p = 0.005), but there was no difference with exercise. At rest, only 2 (1.1%) patients had moderate MR, and none developed severe MR. Pulmonary vascular resistance was higher, and right ventricular (RV)-PA coupling was more impaired in patients with HFpEF and MR at rest and exercise. LV and LA myocardial dysfunction remained more severe in patients with MR during stress compared to those without MR, characterized by greater LA dilatation during all stages of exertion, lower LA emptying fraction and compliance, steeper and rightward-shifted LA pressure-volume relationships, and reduced LV longitudinal contractile function.
Conclusions: Patients with HFpEF and mild or moderate MR have more severe LV systolic dysfunction, LA myopathy, RV-PA uncoupling, and more severe pulmonary vascular disease. Mitral valve incompetence in this setting is a phenotypic marker of more advanced disease but is not a causal factor in development of HFpEF.
Keywords: Echocardiography; Exercise; Haemodynamics; Heart failure with preserved ejection fraction; Mitral regurgitation.
© 2024 European Society of Cardiology.
Figures


References
-
- Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Bohm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med. 2021. doi: 10.1056/NEJMoa2107038 - DOI
-
- Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022. doi: 10.1056/NEJMoa2206286 - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
