

Time to SARS-CoV-2 clearance in African, Caucasian, and Asian ethnic groups
- PMID: 38838076
- PMCID: PMC11150056
- DOI: 10.1111/irv.13238
Time to SARS-CoV-2 clearance in African, Caucasian, and Asian ethnic groups
Abstract
Background: COVID-19 may become a seasonal disease. SARS-CoV-2 active circulation coupled with vaccination efforts has undoubtedly modified the virus dynamic. It is therefore important investigate SARS-CoV-2 dynamic in different groups of population following the course of spatiotemporal variance and immunization.
Methods: To investigate SARS-CoV-2 clearance in different ethnic groups and the impact of immunization, we recruited 777 SARS-CoV-2-positive patients (570 Africans, 156 Caucasians, and 51 Asians). Participants were followed and regularly tested for 2 months until they had two negative tests.
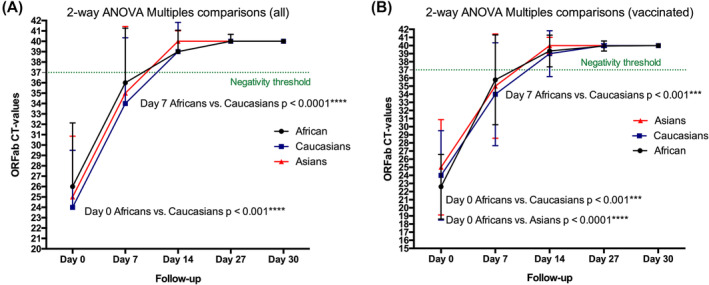
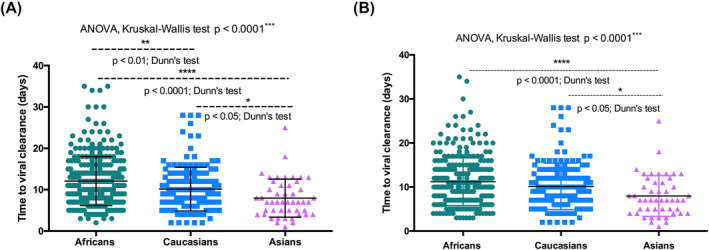
Results: The vaccination rate was 64.6%. African individuals were less symptomatic (2%), Caucasians (41%) and Asians (36.6%). On average, viral clearance occurred after 10.5 days. Viral load at diagnosis was inversely correlated with viral clearance (p < 0.0001). The time of SARS-CoV-2 clearance was higher in Africans and Caucasians than in Asians (Dunn's test p < 0.0001 and p < 0.05, respectively). On average, viral clearance occurred within 9.5 days during the second semester (higher rate of vaccination and SARS-CoV-2 exposition), whereas it took 13.6 days during the first semester (lower rate of vaccination and SARS-CoV-2 exposition) (Mann-Whitney t-test p < 0.0001).
Conclusion: In conclusion, ethnicity and spatiotemporal changes including SARS-CoV-2 exposition and immunization affect SARS-CoV-2 clearance.
Keywords: COVID‐19; RT‐PCR; SARS‐CoV‐2 clearance; ethnicity; herd immunity; vaccination.
© 2024 The Authors. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they do not have any competing or conflicts of interest.
Figures



References
-
- Ke R, Sanche S, Romero‐Severson E, Hengartner N. Fast spread of COVID‐19 in Europe and the US suggests the necessity of early, strong and comprehensive interventions. medRxiv. 2020.
-
- World Health Organization . WHO Coronavirus Disease (COVID‐19) Dashboard. 2022. https://covid19.who.int (Accessed 30 September 2022).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
