

Circulating immune-related proteins associated with immune checkpoint inhibitor efficacy in patients with pancreatic ductal adenocarcinoma
- PMID: 38838501
- PMCID: PMC11190466
- DOI: 10.1016/j.esmoop.2024.103489
Circulating immune-related proteins associated with immune checkpoint inhibitor efficacy in patients with pancreatic ductal adenocarcinoma
Abstract
Background: Most patients with pancreatic ductal adenocarcinoma (PDAC) do not benefit from immune checkpoint inhibitor treatment. However, the phase II study CheckPAC (NCT02866383) showed a clinical benefit (CB) rate of 37% and a response rate of 14% in patients with metastatic PDAC receiving stereotactic radiation therapy and nivolumab with or without ipilimumab. Translational studies were initiated to characterize the patients who would benefit from this treatment. Here, we evaluated the association between treatment outcome and 92 circulating immuno-oncology-related proteins in patients from the CheckPAC trial.
Materials and methods: The study included 78 patients with chemoresistant metastatic PDAC treated with nivolumab ± ipilimumab combined with radiotherapy. Proteins were measured in serum samples collected at baseline and on treatment with the use of the Olink Target 96 Immuno-Oncology panel. A cohort of 234 patients with metastatic PDAC treated with first-line chemotherapy were also included.
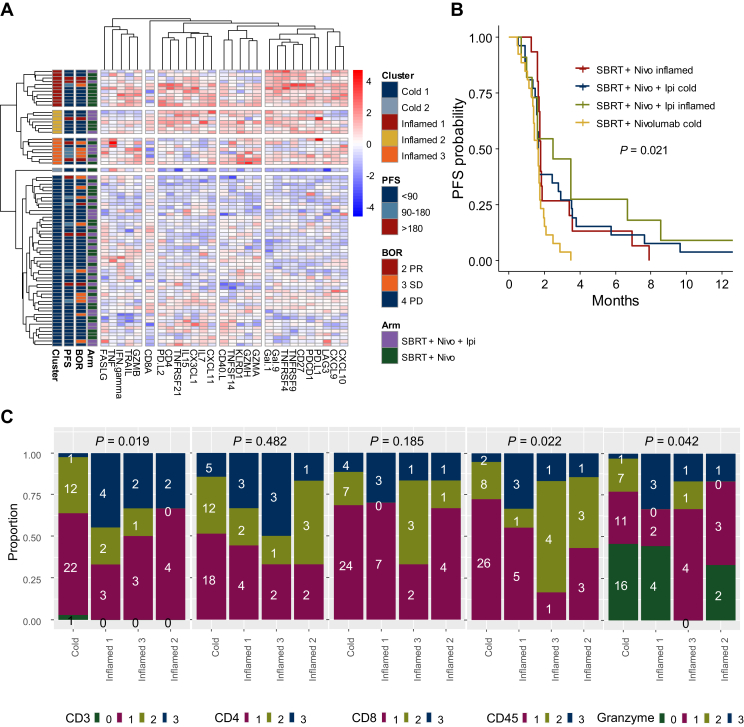
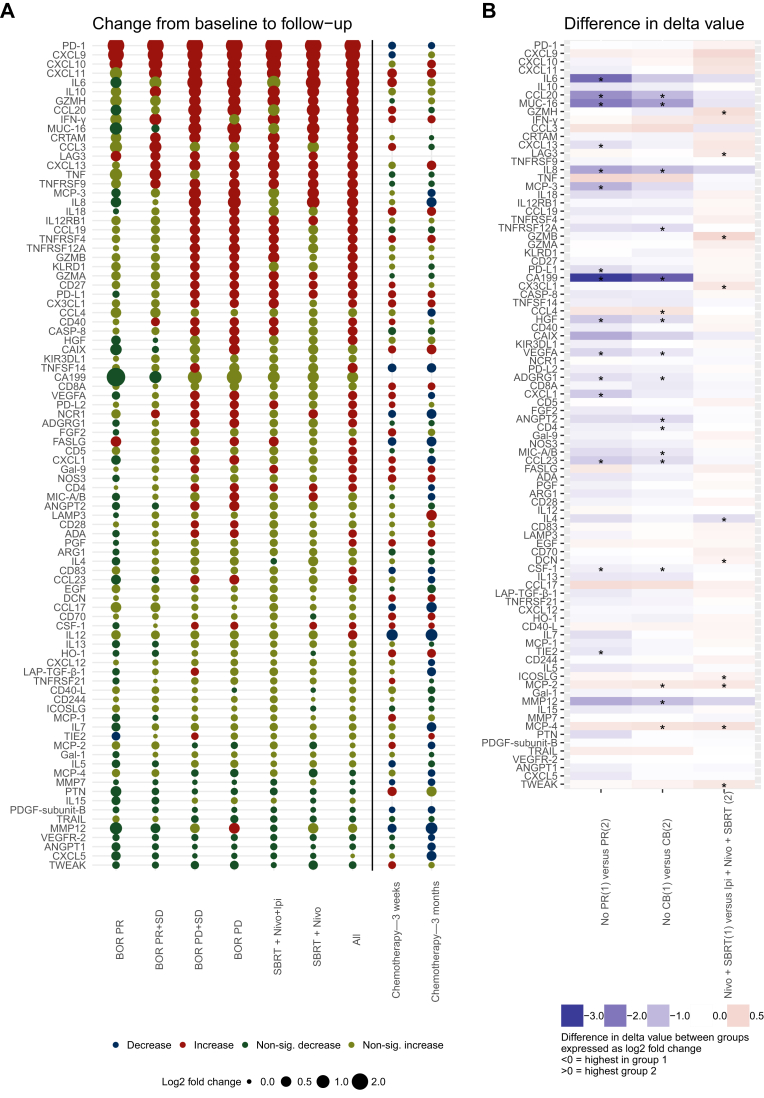
Results: High levels of Fas ligand (FASLG) and galectin 1 (Gal-1) and low levels of C-C motif chemokine 4 were associated with CB. High FASLG and Gal-1 were associated with longer progression-free survival in univariable analysis. In the multivariable Cox regression analysis, the association was significant for Gal-1 (P < 0.001) but not significant for FASLG (P = 0.06). A focused unsupervised hierarchal clustering analysis, including T-cell activation and immune checkpoint-related proteins, identified clusters of patients with higher CB rate and higher tumor expression of leukocyte or T-cell markers (CD3, CD45, granzyme B). Thirty-six proteins increased significantly during immunotherapy. Several proteins (including FASLG, checkpoint proteins, and immune activation markers) increased independently of response during immunotherapy but did not increase in the cohort of patients treated with chemotherapy.
Conclusions: Circulating levels of immune-related proteins like FASLG and Gal-1 might be used to predict the efficacy of checkpoint inhibitors in patients with metastatic PDAC.
Keywords: biomarkers; circulating proteins; immune checkpoint inhibitor; immuno-oncology; pancreatic cancer.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Siegel R.L., Miller K.D., Wagle N.S., Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. - PubMed
-
- Mizrahi J.D., Surana R., Valle J.W., Shroff R.T. Pancreatic cancer. Lancet. 2020;395(10242):2008–2020. - PubMed
-
- Conroy T., Desseigne F., Ychou M., et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. - PubMed
-
- Wang-Gillam A., Li C.P., Bodoky G., et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): a global, randomised, open-label, phase 3 trial. Lancet. 2016;387(10018):545–557. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
