

Clonal hematopoiesis driven by mutated DNMT3A promotes inflammatory bone loss
- PMID: 38838669
- PMCID: PMC11246233
- DOI: 10.1016/j.cell.2024.05.003
Clonal hematopoiesis driven by mutated DNMT3A promotes inflammatory bone loss
Abstract
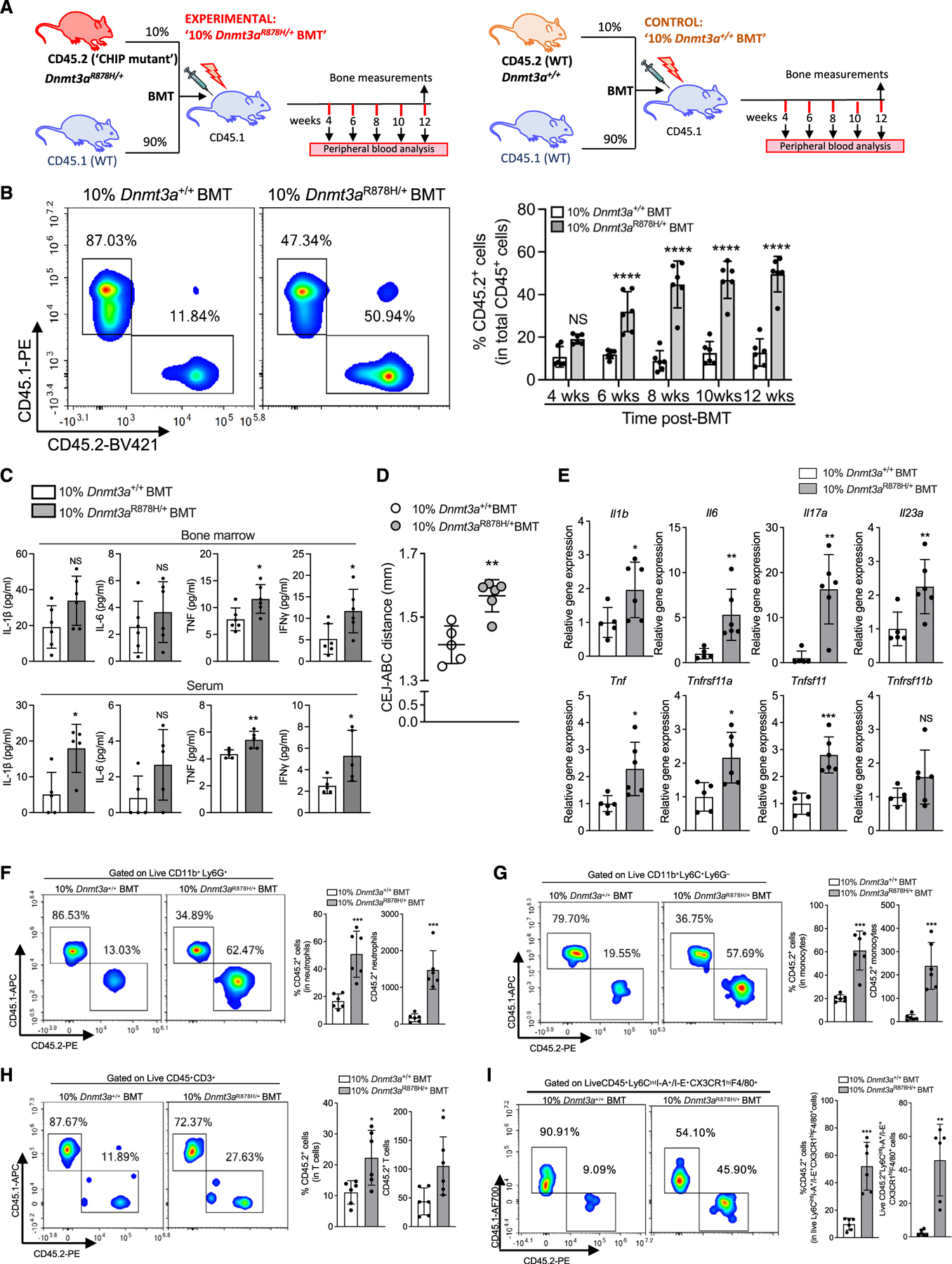
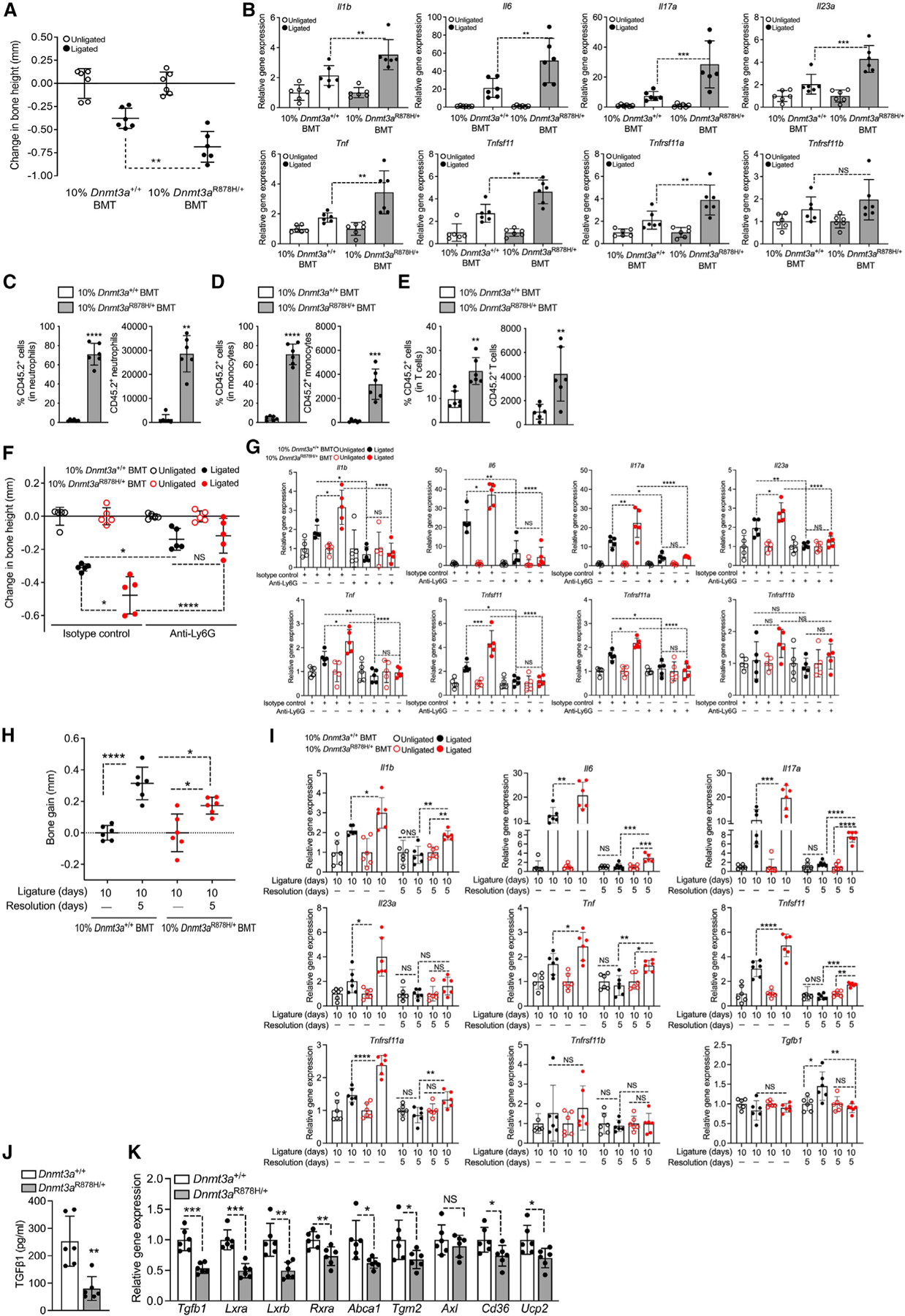
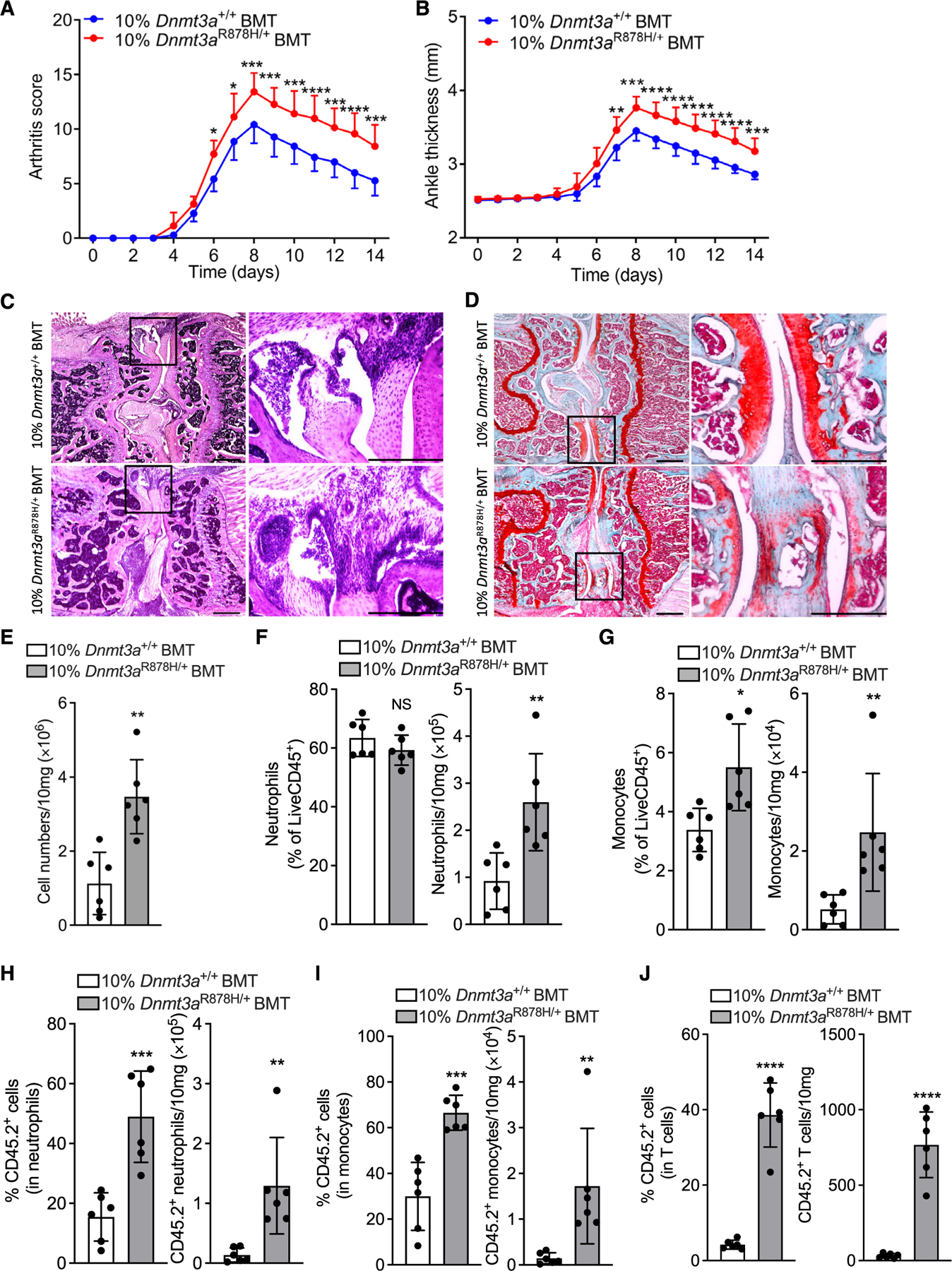
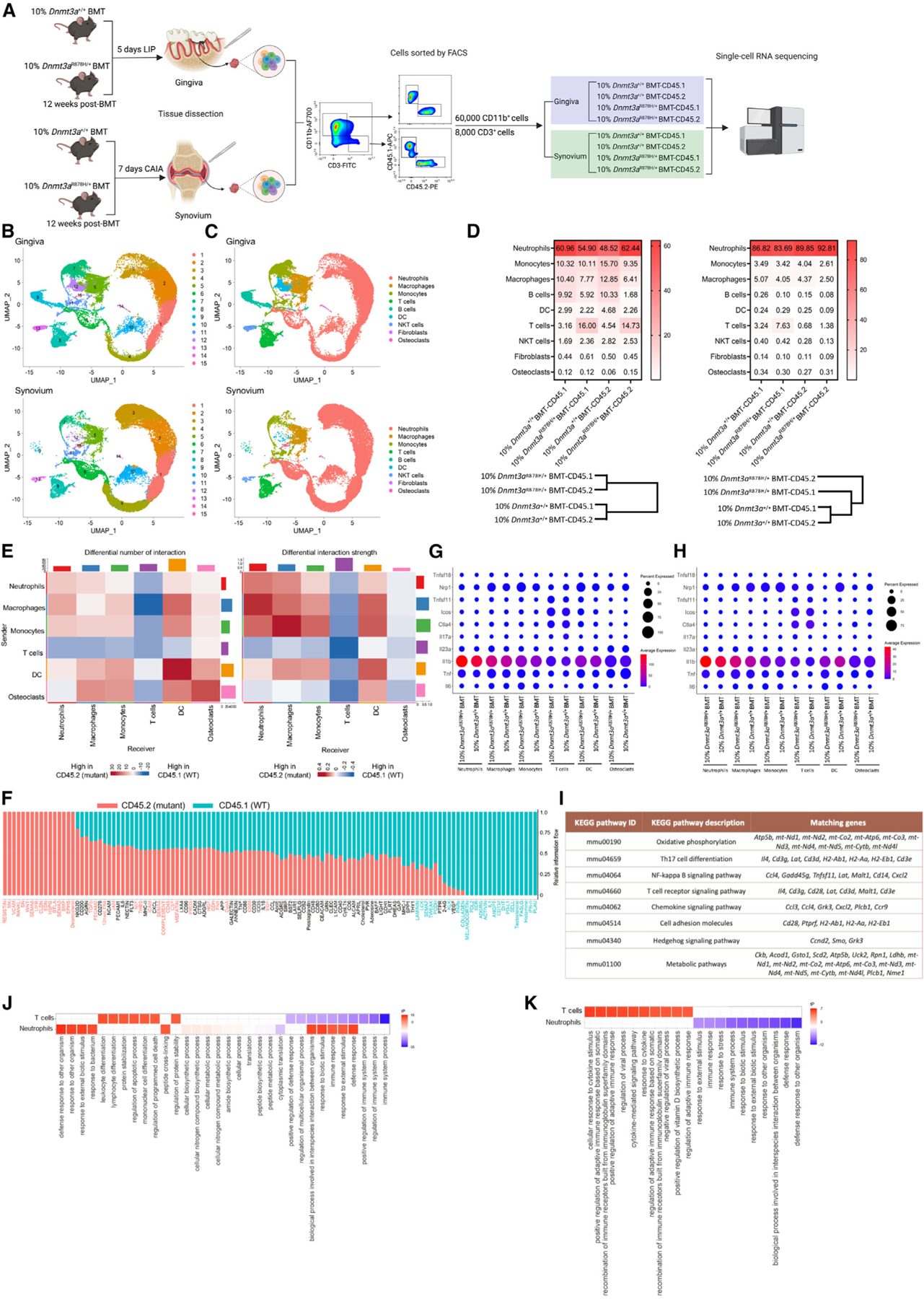
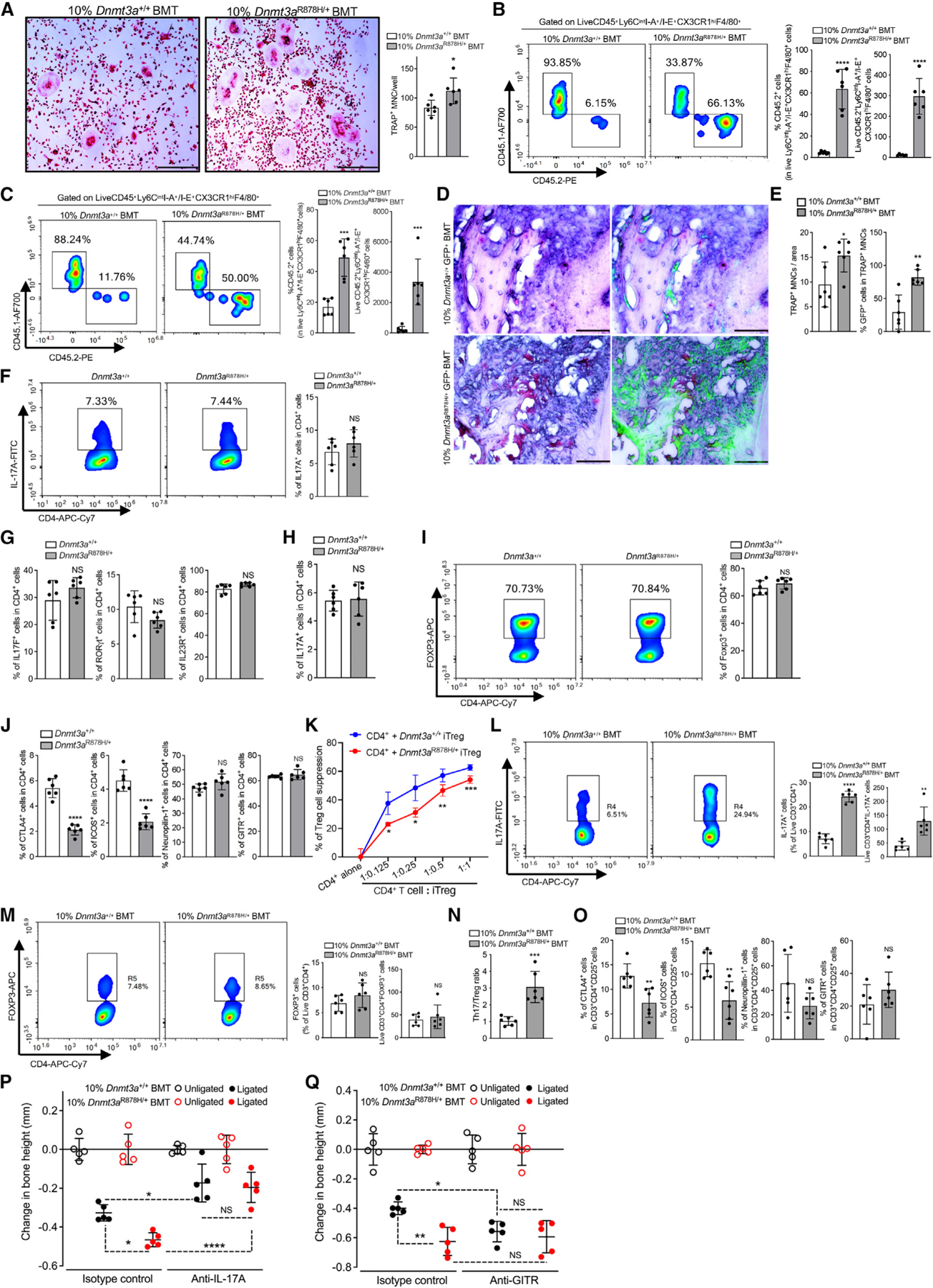
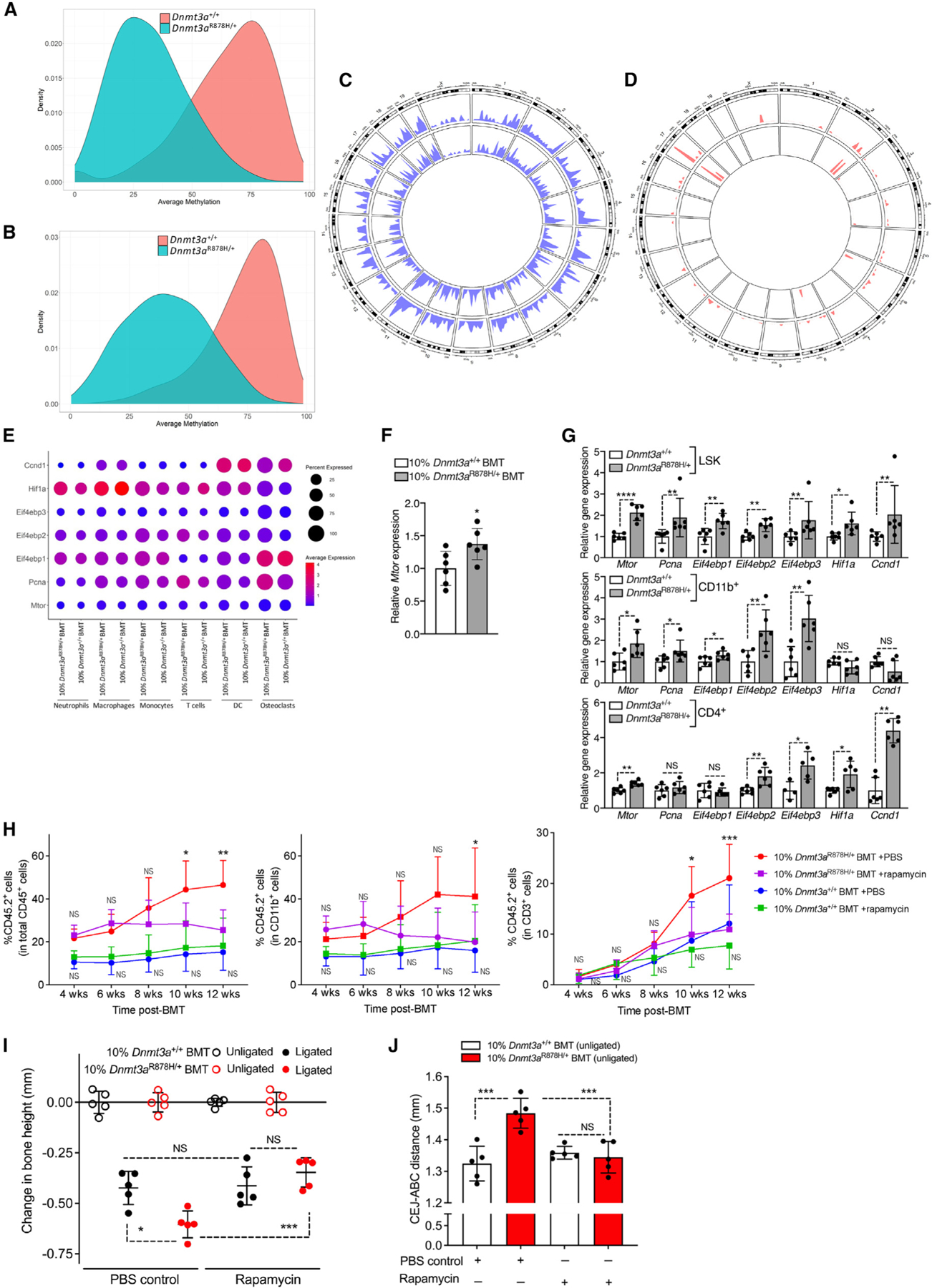
Clonal hematopoiesis of indeterminate potential (CHIP) arises from aging-associated acquired mutations in hematopoietic progenitors, which display clonal expansion and produce phenotypically altered leukocytes. We associated CHIP-DNMT3A mutations with a higher prevalence of periodontitis and gingival inflammation among 4,946 community-dwelling adults. To model DNMT3A-driven CHIP, we used mice with the heterozygous loss-of-function mutation R878H, equivalent to the human hotspot mutation R882H. Partial transplantation with Dnmt3aR878H/+ bone marrow (BM) cells resulted in clonal expansion of mutant cells into both myeloid and lymphoid lineages and an elevated abundance of osteoclast precursors in the BM and osteoclastogenic macrophages in the periphery. DNMT3A-driven clonal hematopoiesis in recipient mice promoted naturally occurring periodontitis and aggravated experimentally induced periodontitis and arthritis, associated with enhanced osteoclastogenesis, IL-17-dependent inflammation and neutrophil responses, and impaired regulatory T cell immunosuppressive activity. DNMT3A-driven clonal hematopoiesis and, subsequently, periodontitis were suppressed by rapamycin treatment. DNMT3A-driven CHIP represents a treatable state of maladaptive hematopoiesis promoting inflammatory bone loss.
Keywords: DNMT3A; T cells; arthritis; bone marrow; clonal hematopoiesis of indeterminate potential; hematopoietic stem and progenitor cells; inflammation; neutrophils; osteoclastogenesis; periodontitis.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests P.N. reports research grants from Allelica, Amgen, Apple, Boston Scientific, Genentech/Roche, and Novartis, personal fees from Allelica, Apple, AstraZeneca, Blackstone Life Sciences, Creative Education Concepts, CRISPR Therapeutics, Eli Lilly & Co, Foresite Labs, Genentech/Roche, GV, HeartFlow, Magnet Biomedicine, Merck, and Novartis, scientific advisory board membership of Esperion Therapeutics, Preciseli, and TenSixteen Bio, scientific co-founder of TenSixteen Bio, equity in MyOme, Preciseli, and TenSixteen Bio, and spousal employment at Vertex Pharmaceuticals, all unrelated to the present work. M.G.N. is an advisory board member of Cell and scientific founder of Lemba, TTxD, and Biotrip.
Figures
Similar articles
-
Selective advantage of mutant stem cells in human clonal hematopoiesis is associated with attenuated response to inflammation and aging.Cell Stem Cell. 2024 Aug 1;31(8):1127-1144.e17. doi: 10.1016/j.stem.2024.05.010. Epub 2024 Jun 24. Cell Stem Cell. 2024. PMID: 38917807 Free PMC article.
-
Sex differences in DNMT3A-mutant clonal hematopoiesis and the effects of estrogen.Cell Rep. 2025 Apr 22;44(4):115494. doi: 10.1016/j.celrep.2025.115494. Epub 2025 Apr 2. Cell Rep. 2025. PMID: 40178977
-
Metformin reduces the competitive advantage of Dnmt3aR878H HSPCs.Nature. 2025 Jun;642(8067):421-430. doi: 10.1038/s41586-025-08871-w. Epub 2025 Apr 16. Nature. 2025. PMID: 40240595
-
Clonal hematopoiesis and associated diseases: A review of recent findings.Cancer Sci. 2021 Oct;112(10):3962-3971. doi: 10.1111/cas.15094. Epub 2021 Aug 12. Cancer Sci. 2021. PMID: 34328684 Free PMC article. Review.
-
Clonal hematopoiesis of indeterminate potential (CHIP): A potential contributor to lymphoma.Crit Rev Oncol Hematol. 2025 Feb;206:104589. doi: 10.1016/j.critrevonc.2024.104589. Epub 2024 Dec 10. Crit Rev Oncol Hematol. 2025. PMID: 39667716 Review.
Cited by
-
Elevated mitochondrial membrane potential is a therapeutic vulnerability in Dnmt3a-mutant clonal hematopoiesis.Nat Commun. 2025 Apr 16;16(1):3306. doi: 10.1038/s41467-025-57238-2. Nat Commun. 2025. PMID: 40240771 Free PMC article.
-
ASXL1 mutation-related clonal hematopoiesis and age-related diseases: clinical evidence and molecular insights.Int J Hematol. 2025 Aug 7. doi: 10.1007/s12185-025-04038-5. Online ahead of print. Int J Hematol. 2025. PMID: 40773119 Review.
-
Clonal hematopoiesis of indeterminate potential (CHIP) in cerebromicrovascular aging: implications for vascular contributions to cognitive impairment and dementia (VCID).Geroscience. 2025 Jun;47(3):2739-2775. doi: 10.1007/s11357-025-01654-1. Epub 2025 Apr 11. Geroscience. 2025. PMID: 40214958 Free PMC article. Review.
-
Trained immunity in chronic inflammatory diseases and cancer.Nat Rev Immunol. 2025 Jul;25(7):497-514. doi: 10.1038/s41577-025-01132-x. Epub 2025 Jan 31. Nat Rev Immunol. 2025. PMID: 39891000 Review.
-
Implications of Clonal Hematopoiesis in Hematological and Non-Hematological Disorders.Cancers (Basel). 2024 Dec 9;16(23):4118. doi: 10.3390/cancers16234118. Cancers (Basel). 2024. PMID: 39682303 Free PMC article. Review.
References
MeSH terms
Substances
Grants and funding
- RC2 HL102419/HL/NHLBI NIH HHS/United States
- P30 ES010126/ES/NIEHS NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- R01 HL059367/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- U01 DE025046/DE/NIDCR NIH HHS/United States
- R01 HL087641/HL/NHLBI NIH HHS/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
- R01 DE021418/DE/NIDCR NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- R01 DE011551/DE/NIDCR NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- R01 DE031206/DE/NIDCR NIH HHS/United States
- U01 HG004402/HG/NHGRI NIH HHS/United States
- U54 HG003273/HG/NHGRI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- R01 DE033643/DE/NIDCR NIH HHS/United States
- UM1 HG008898/HG/NHGRI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
