

Waist-to-height ratio and body fat percentage as risk factors for ischemic cardiovascular disease: a prospective cohort study from UK Biobank
- PMID: 38839194
- PMCID: PMC11196863
- DOI: 10.1016/j.ajcnut.2024.03.018
Waist-to-height ratio and body fat percentage as risk factors for ischemic cardiovascular disease: a prospective cohort study from UK Biobank
Erratum in
-
Corrigendum to "Waist-to-height ratio and body fat percentage as risk factors for ischemic cardiovascular disease: a prospective cohort study from UK Biobank" [Am J Clin Nutr 119 (2024) 1386-1396].Am J Clin Nutr. 2024 Sep;120(3):758. doi: 10.1016/j.ajcnut.2024.07.011. Epub 2024 Jul 20. Am J Clin Nutr. 2024. PMID: 39038614 Free PMC article. No abstract available.
Abstract
Background: The independent effect of waist-to-height ratio (WHtR) and body fat percentage (BF%) on ischemic cardiovascular disease (CVD) remains uncertain.
Objectives: This study aimed to investigate the independent associations of WHtR and BF% with ischemic CVD.
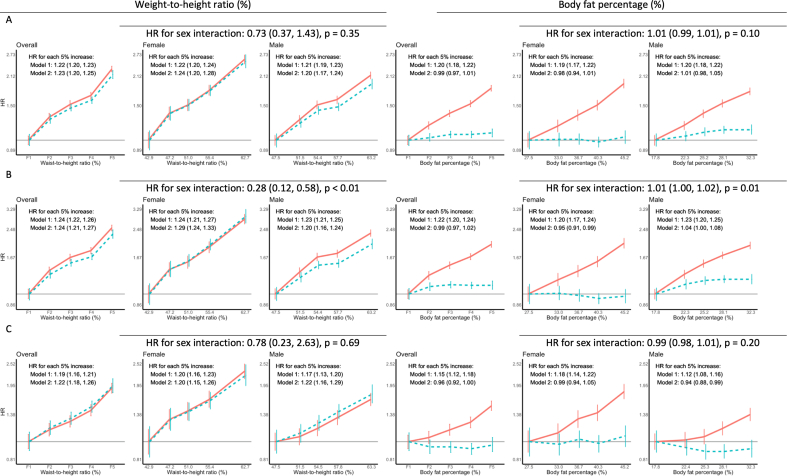
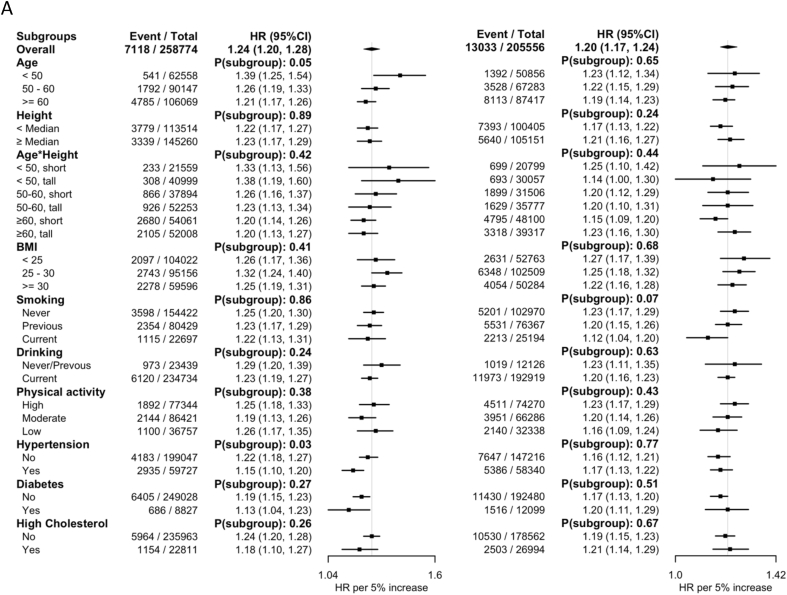
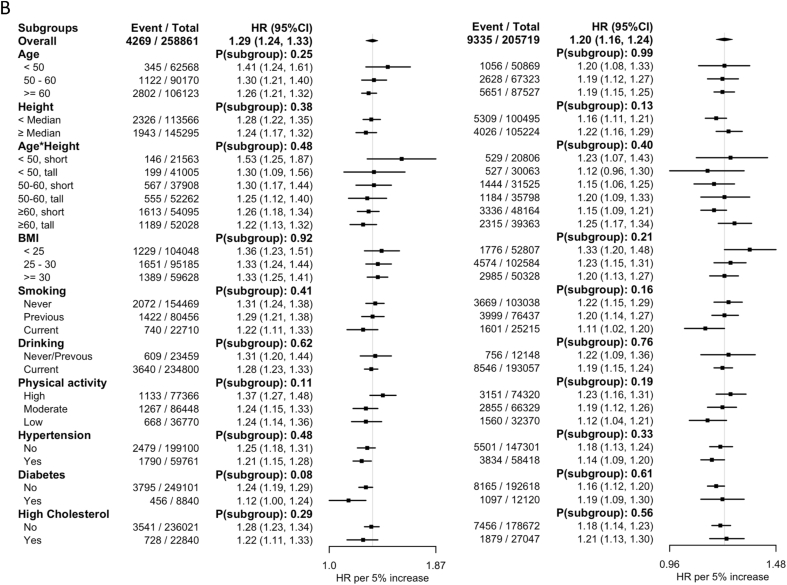
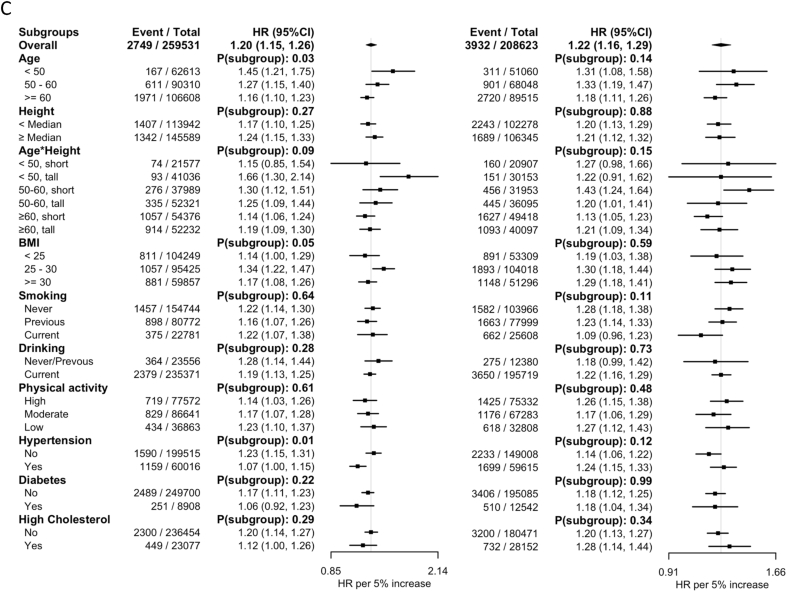
Methods: This prospective cohort study used data from the UK Biobank. BF% was calculated as fat mass divided by body weight, measured by bioimpedance. Cox models estimated hazard ratios (HRs) with 95% confidence intervals (CIs) for overall and sex-specific associations of BF% and WHtR with risks of ischemic CVD and its main subtypes [myocardial infarction (MI) and ischemic stroke (IS)], adjusted for a range of potential confounders, including mutual adjustment for BF% and WHtR.
Results: In total, 468,333 participants without existing CVD were included in the analysis. During 12 y of follow-up, 20,151 ischemic CVD events, 13,604 MIs, and 6681 ISs were recorded. WHtR was linearly associated with ischemic CVD, MI, and IS, with an HR per 5% increase of 1.23 (95% CI: 1.20, 1.25), 1.24 (95% CI: 1.21, 1.27), and 1.22 (95% CI: 1.18, 1.26), respectively, independent of BF%. A stronger association between WHtR and MI was seen in females than in males. The association of BF% with these outcomes was substantially attenuated in both sexes after adjustment for WHtR. For example, in females, the HR (highest compared with lowest fifth) was reduced from 1.94 (95% CI: 1.76, 2.15) to 1.04 (95% CI: 0.90, 1.01) for ischemic CVD, from 2.04 (95% CI: 1.79, 2.32) to 0.97 (95% CI: 0.81, 1.16) for MI, and from 1.81 (95% CI: 1.54, 2.13) to 1.07 (95% CI: 0.85, 1.33) for IS.
Conclusions: WHtR, when used as a proxy measure for central obesity, is linearly associated with ischemic CVD in both sexes, which is independent of BF%. In contrast, the relationship of BF% with these health outcomes is predominantly driven by its correlation with WHtR.
Keywords: UK Biobank; body fat percentage; ischemic cardiovascular diseases; ischemic stroke; myocardial infarction; waist-to-height ratio.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest MW does consultancy for Amgen and Freeline outside the submitted work; no support from any organization for the submitted work; no other relationships or activities that could appear to have influenced the submitted work. All other authors report no conflicts of interests.
Figures
Comment in
-
People with normal waist circumference but with elevated waist-to-height ratio: an overlooked population with increased cardiometabolic risk?Am J Clin Nutr. 2024 Jun;119(6):1379-1380. doi: 10.1016/j.ajcnut.2024.04.013. Epub 2024 May 9. Am J Clin Nutr. 2024. PMID: 38839192 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
