

X‑chromosome loss rescues Sertoli cell maturation and spermatogenesis in Klinefelter syndrome
- PMID: 38839795
- PMCID: PMC11153587
- DOI: 10.1038/s41419-024-06792-6
X‑chromosome loss rescues Sertoli cell maturation and spermatogenesis in Klinefelter syndrome
Abstract
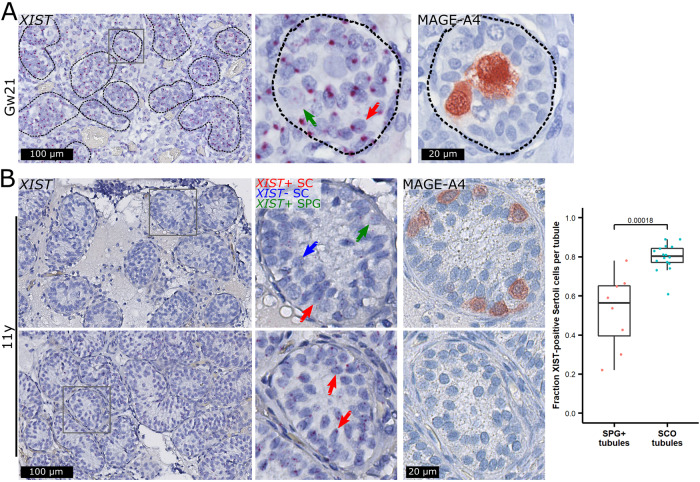
Klinefelter syndrome (47,XXY) causes infertility with a testicular histology comprising two types of Sertoli cell-only tubules, representing mature and immature-like Sertoli cells, and occasionally focal spermatogenesis. Here, we show that the immature-like Sertoli cells highly expressed XIST and had two X-chromosomes, while the mature Sertoli cells lacked XIST expression and had only one X-chromosome. Sertoli cells supporting focal spermatogenesis also lacked XIST expression and the additional X-chromosome, while the spermatogonia expressed XIST despite having only one X-chromosome. XIST was expressed in Sertoli cells until puberty, where a gradual loss was observed. Our results suggest that a micro-mosaic loss of the additional X-chromosome is needed for Sertoli cells to mature and to allow focal spermatogenesis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Berglund A, Viuff MH, Skakkebæk A, Chang S, Stochholm K, Gravholt CH. Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47,XXX and 47,XYY syndrome: A nationwide cohort study 11 Medical and Health Sciences 1117 Public Health and Health Services. Orphanet J Rare Dis. 2019;14:1–9. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
