

Real-time predictive model of extrauterine growth retardation in preterm infants with gestational age less than 32 weeks
- PMID: 38839838
- PMCID: PMC11153599
- DOI: 10.1038/s41598-024-63593-9
Real-time predictive model of extrauterine growth retardation in preterm infants with gestational age less than 32 weeks
Abstract
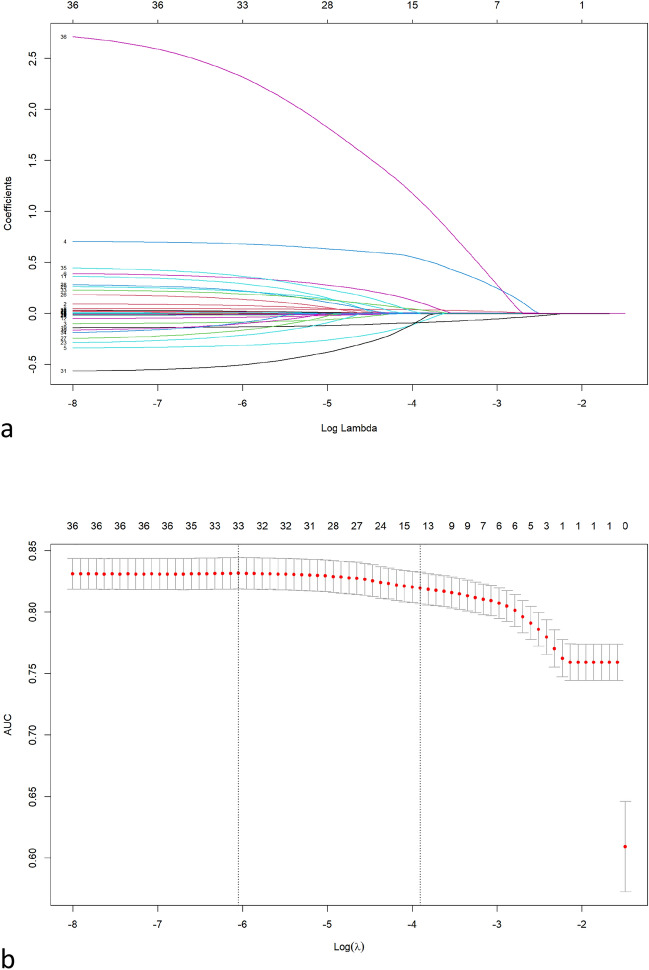
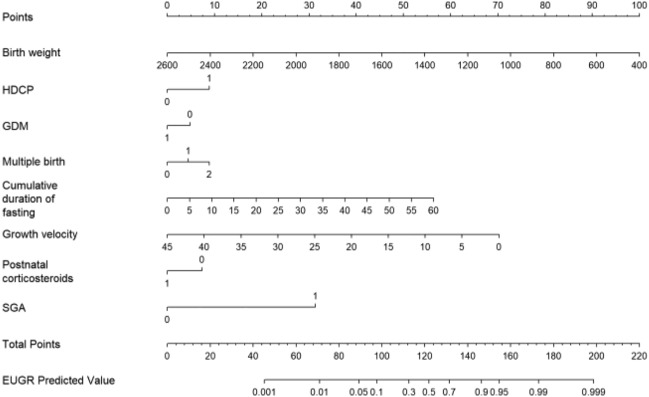
The aim of this study was to develop a real-time risk prediction model for extrauterine growth retardation (EUGR). A total of 2514 very preterm infants were allocated into a training set and an external validation set. The most appropriate independent variables were screened using univariate analysis and Lasso regression with tenfold cross-validation, while the prediction model was designed using binary multivariate logistic regression. A visualization of the risk variables was created using a nomogram, while the calibration plot and receiver operating characteristic (ROC) curves were used to calibrate the prediction model. Clinical efficacy was assessed using the decision curve analysis (DCA) curves. Eight optimal predictors that namely birth weight, small for gestation age (SGA), hypertensive disease complicating pregnancy (HDCP), gestational diabetes mellitus (GDM), multiple births, cumulative duration of fasting, growth velocity and postnatal corticosteroids were introduced into the logistic regression equation to construct the EUGR prediction model. The area under the ROC curve of the training set and the external verification set was 83.1% and 84.6%, respectively. The calibration curve indicate that the model fits well. The DCA curve shows that the risk threshold for clinical application is 0-95% in both set. Introducing Birth weight, SGA, HDCP, GDM, Multiple births, Cumulative duration of fasting, Growth velocity and Postnatal corticosteroids into the nomogram increased its usefulness for predicting EUGR risk in very preterm infants.
Keywords: Extrauterine growth retardation; Nomogram; Prediction; Very preterm infant.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Multicenter Study Collaborative Group for Evaluation of Outcomes in Very Low Birth Weight Infants Risk factors for extrauterine growth retardation in very low birth weight infants: A multicenter study. Zhonghua Er Ke Za Zhi. 2020;58(8):653–660. doi: 10.3760/cma.j.cn112140-20200326-00308. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
