

Thromboembolic events and vascular dementia in patients with atrial fibrillation and low apparent stroke risk
- PMID: 38839900
- PMCID: PMC11333279
- DOI: 10.1038/s41591-024-03049-9
Thromboembolic events and vascular dementia in patients with atrial fibrillation and low apparent stroke risk
Abstract
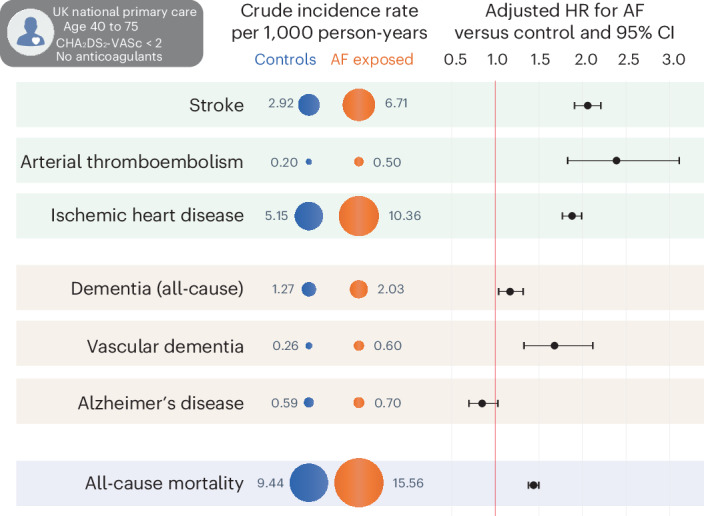
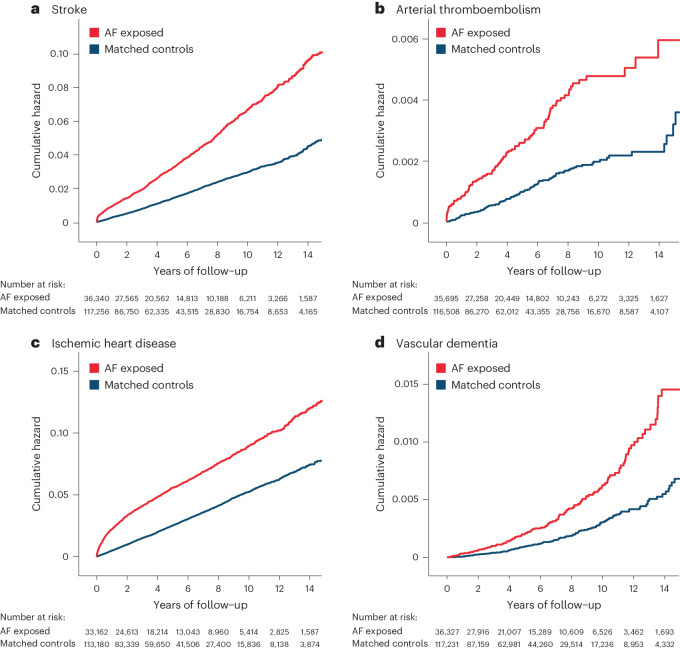
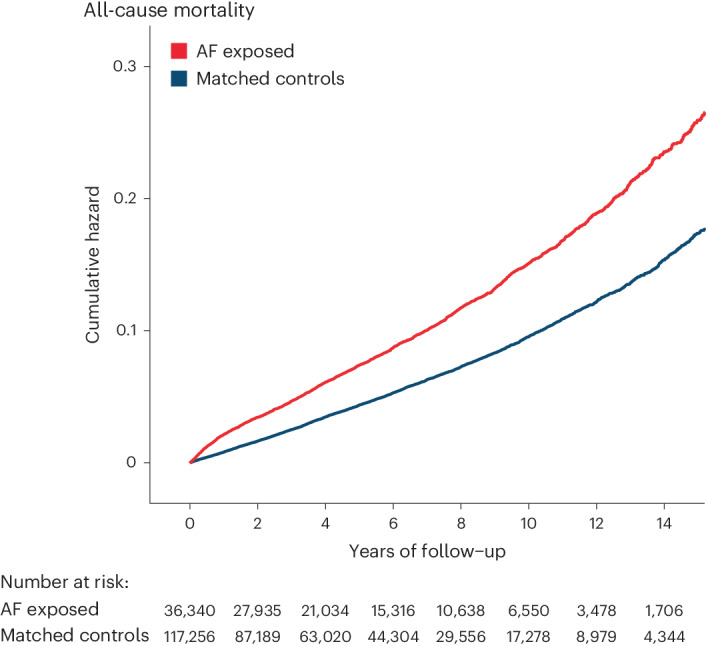
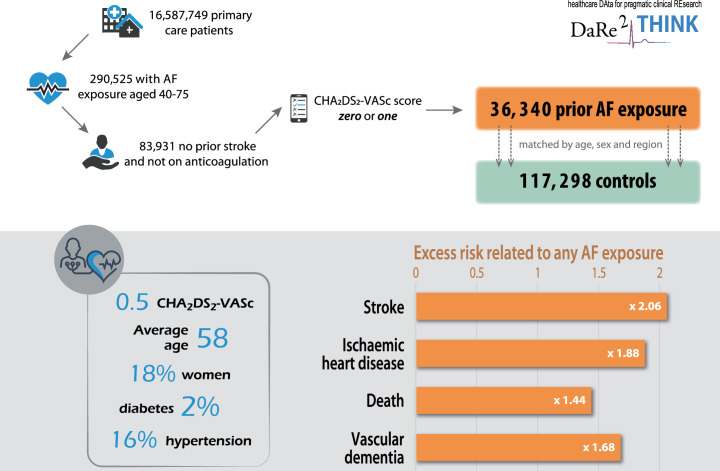
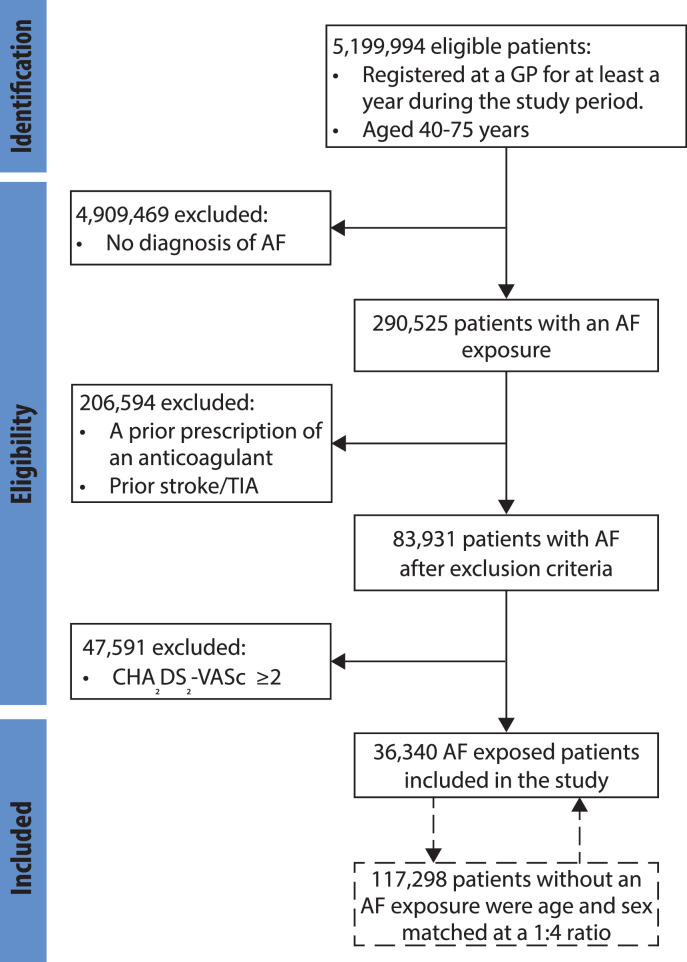
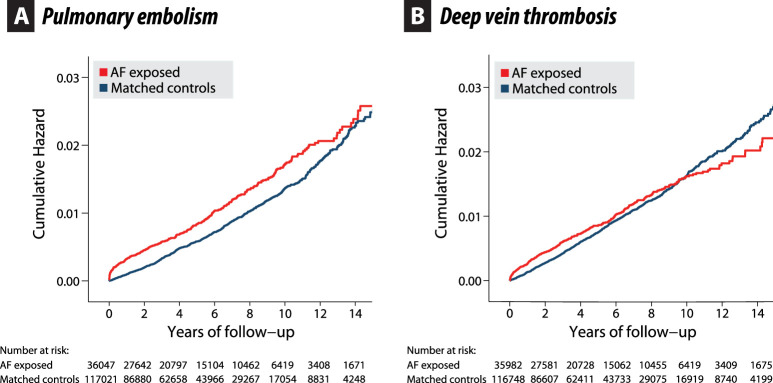
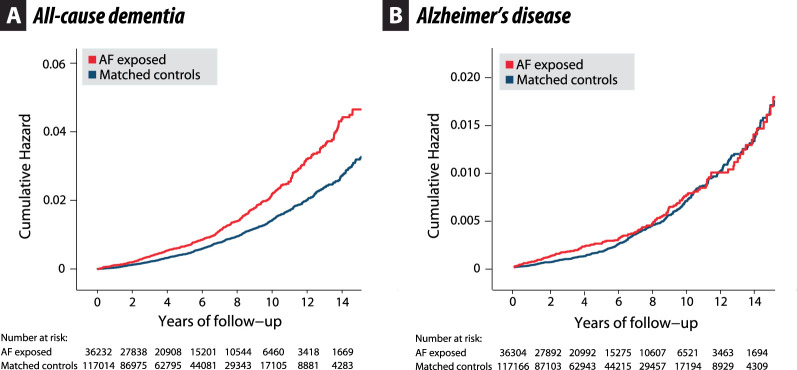
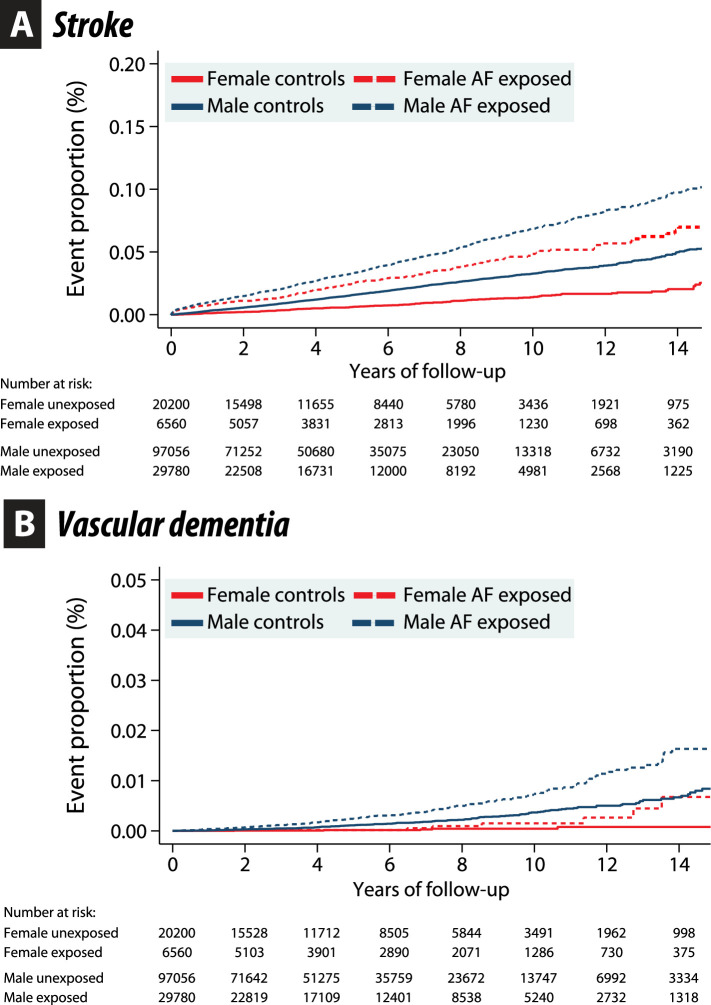
The prevention of thromboembolism in atrial fibrillation (AF) is typically restricted to patients with specific risk factors and ignores outcomes such as vascular dementia. This population-based cohort study used electronic healthcare records from 5,199,994 primary care patients (UK; 2005-2020). A total of 290,525 (5.6%) had a diagnosis of AF and were aged 40-75 years, of which 36,340 had no history of stroke, a low perceived risk of stroke based on clinical risk factors and no oral anticoagulant prescription. Matching was performed for age, sex and region to 117,298 controls without AF. During 5 years median follow-up (831,005 person-years), incident stroke occurred in 3.8% with AF versus 1.5% control (adjusted hazard ratio (HR) 2.06, 95% confidence interval (CI) 1.91-2.21; P < 0.001), arterial thromboembolism 0.3% versus 0.1% (HR 2.39, 95% CI 1.83-3.11; P < 0.001), and all-cause mortality 8.9% versus 5.0% (HR 1.44, 95% CI 1.38-1.50; P < 0.001). AF was associated with all-cause dementia (HR 1.17, 95% CI 1.04-1.32; P = 0.010), driven by vascular dementia (HR 1.68, 95% CI 1.33-2.12; P < 0.001) rather than Alzheimer's disease (HR 0.85, 95% CI 0.70-1.03; P = 0.09). Death and thromboembolic outcomes, including vascular dementia, are substantially increased in patients with AF despite a lack of conventional stroke risk factors.
© 2024. The Author(s).
Conflict of interest statement
The post of A.R.M. is funded by The Cook and Wolstenholme Charitable Trust (charity no. 1091984), EU Horizon and UKRI (HYPERMARKER 101095480) and UK NHS (Data for R&D) Subnational Secure Data Environment program. A.S. has no declarations during the study period; after the study was completed she left the University of Birmingham to take a post at AstraZeneca. A.C., X.W., P. Myles and P. McGreavy declare no competing interests. K.V.B. reports a BHF Career Development Research Fellowship (for nurses and healthcare professionals) FS/CDRF/21/21032 and Membership of the British Society of Echocardiography education committee. D.S. reports grants from NIHR (130280), during the conduct of the study and grants from Pfizer outside the submitted work. K.N. reports grants from NIHR, during the conduct of the study and research grants from UKRI/MRC, Kennedy Trust for Rheumatology Research, Health Data Research UK, Wellcome Trust, European Regional Development Fund, Institute for Global Innovation, Boehringer Ingelheim, Action Against Macular Degeneration Charity, Midlands Neuroscience Teaching and Development Funds, South Asian Health Foundation, Vifor Pharma, College of Police and CSL Behring, outside the submitted work; and consulting fees from Boehringer Ingelheim, Sanofi, CEGEDIM and MSD; and holds a leadership/fiduciary role with NICST, a charity and OpenClinical, a Social Enterprise; outside the submitted work. D.K. reports grants from the NIHR (CDF-2015-08-074 RATE-AF; NIHR130280 DaRe2THINK; NIHR132974 DaRe2THINK-NeuroVascular; NIHR203326 Biomedical Research Centre), the British Heart Foundation (PG/17/55/33087, AA/18/2/34218 and FS/CDRF/21/21032), the EU/EFPIA Innovative Medicines Initiative (BigData@Heart 116074), EU Horizon and UKRI (HYPERMARKER 101095480), UK NHS (Data for R&D) Subnational Secure Data Environment program, UK Dept. for Business, Energy & Industrial Strategy Regulators Pioneer Fund, the Cook & Wolstenholme Charitable Trust and the ESC supported by educational grants from Boehringer Ingelheim/BMS-Pfizer Alliance/Bayer/Daiichi Sankyo/Boston Scientific, the NIHR/University of Oxford Biomedical Research Centre and British Heart Foundation/University of Birmingham Accelerator Award (STEEER-AF). In addition, D.K. has received research grants and advisory board fees from Bayer, Amomed and Protherics Medicines Development, all outside the submitted work.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
