

Patient-reported outcomes and treatment adherence in type 2 diabetes using natural language processing: Wave 8 of the Observational International Diabetes Management Practices Study
- PMID: 38840439
- PMCID: PMC11363103
- DOI: 10.1111/jdi.14228
Patient-reported outcomes and treatment adherence in type 2 diabetes using natural language processing: Wave 8 of the Observational International Diabetes Management Practices Study
Abstract
Aims/introduction: We analyzed patient-reported outcomes of people with type 2 diabetes to better understand perceptions and experiences contributing to treatment adherence.
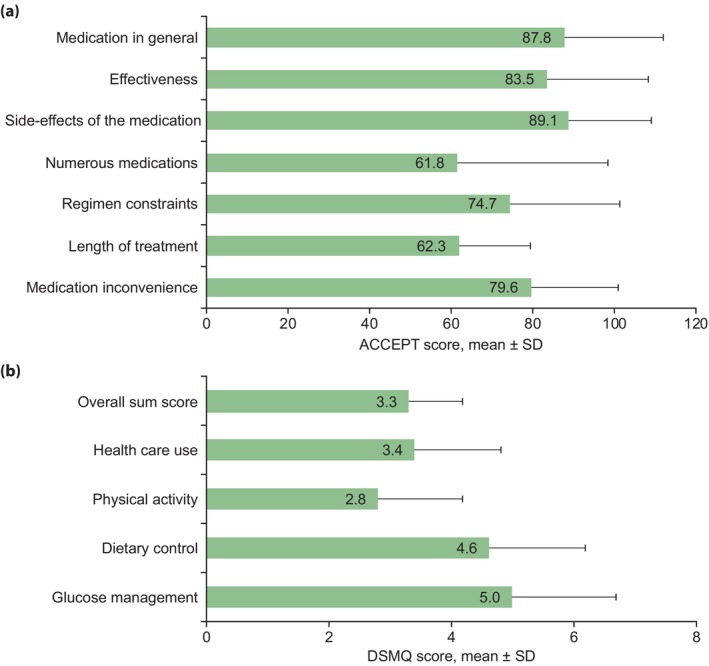
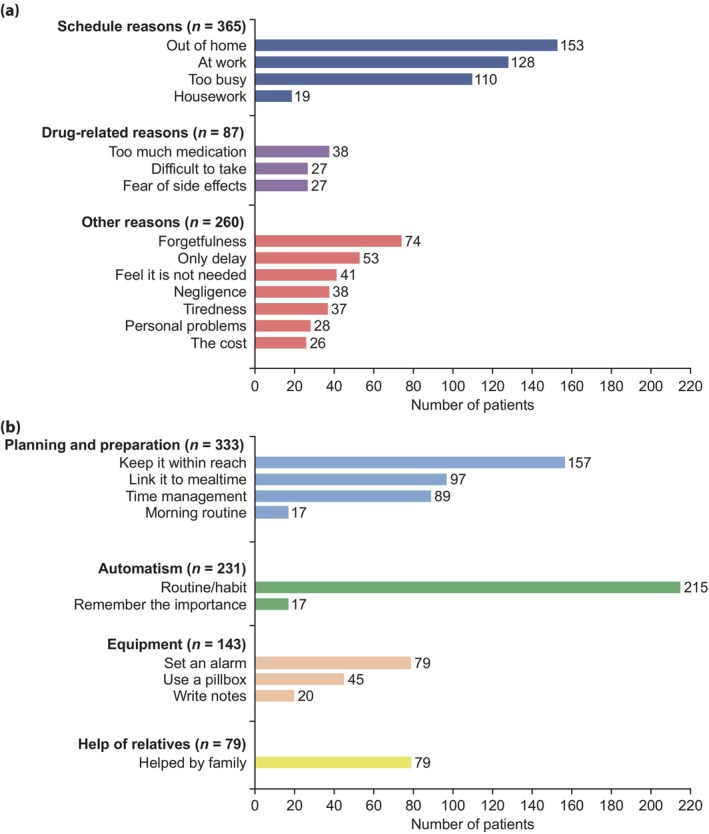
Materials and methods: In the ongoing International Diabetes Management Practices Study, we collected patient-reported outcomes data from structured questionnaires (chronic treatment acceptance questionnaire and Diabetes Self-Management Questionnaire) and free-text answers to open-ended questions to assess perceptions of treatment value and side-effects, as well as barriers to, and enablers for, adherence and self-management. Free-text answers were analyzed by natural language processing.
Results: In 2018-2020, we recruited 2,475 patients with type 2 diabetes (43.3% insulin-treated, glycated hemoglobin (HbA1c) 8.0 ± 1.8%; 30.9% with HbA1c <7%) from 13 countries across Africa, the Middle East, Europe, Latin America and Asia. Mean ± standard deviation scores of chronic treatment acceptance questionnaire (acceptance of medication, rated out of 100) and Diabetes Self-Management Questionnaire (self-management, rated out of 10) were 87.8 ± 24.5 and 3.3 ± 0.9, respectively. Based on free-text analysis and coded responses, one in three patients reported treatment non-adherence. Overall, although most patients accepted treatment values and side-effects, self-management was suboptimal. Treatment duration, regimen complexity and disruption of daily routines were major barriers to adherence, whereas habit formation was a key enabler. Treatment-adherent patients were older (60 ± 11.6 vs 55 ± 11.7 years, P < 0.001), and more likely to have longer disease duration (12 ± 8.6 vs 10 ± 7.7 years, P < 0.001), exposure to diabetes education (73.1% vs 67.8%, P < 0.05), lower HbA1c (7.9 ± 1.8% vs 8.3 ± 1.9%, P < 0.001) and attainment of HbA1c <7% (29.7% vs 23.3%, P < 0.01).
Conclusions: Patient perceptions/experiences influence treatment adherence and self-management. Patient-centered education and support programs that consider patient-reported outcomes aimed at promoting empowerment and developing new routines might improve glycemic control.
Keywords: Clincal; Glycemic control; Patient‐reported outcomes; Treatment - Education; Type 2 diabetes.
© 2024 The Authors. Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
JCNC, JJG, HI, AR, JCM, MS and PA are all members of the IDMPS steering committee, and have received honoraria for travel grants and speakers' fees from Sanofi. JCNC has also received research grants and/or honoraria for consultancy or giving lectures from Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Merck Serono, Merck Sharp & Dohme, Novartis, Pfizer, Servier, Sanofi and Viatris. PA has served as a consultant for and received speaker fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk and Sanofi; and has served on an advisory board for Merck Sharp & Dohme and Sanofi. MR and LD are employees of Quinten, contracted by Sanofi. LMM is an employee of IVIDATA Life Sciences, contracted by Sanofi. JMC is an employee of Sanofi and may hold Sanofi stocks/shares.
Approval of the research protocol: The protocol for this research project has been approved by a suitably constituted Ethics Committee of the institution, and it conforms to the provisions of the Declaration of Helsinki.
Informed consent: Informed consent was obtained from each study participant.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Figures
Similar articles
-
Glycemic Control in Insulin-Treated Patients With Type 2 Diabetes: Empowerment Perceptions and Diabetes Distress as Important Determinants.Biol Res Nurs. 2019 Mar;21(2):182-189. doi: 10.1177/1099800418820170. Epub 2018 Dec 25. Biol Res Nurs. 2019. PMID: 30585081
-
Persistent poor glycaemic control in individuals with type 2 diabetes in developing countries: 12 years of real-world evidence of the International Diabetes Management Practices Study (IDMPS).Diabetologia. 2020 Apr;63(4):711-721. doi: 10.1007/s00125-019-05078-3. Epub 2020 Jan 4. Diabetologia. 2020. PMID: 31901950 Free PMC article.
-
Individualized HbA1c Goals, and Patient Awareness and Attainment of Goals in Type 2 Diabetes Mellitus: A Real-World Multinational Survey.Adv Ther. 2022 Feb;39(2):1016-1032. doi: 10.1007/s12325-021-01985-3. Epub 2021 Dec 24. Adv Ther. 2022. PMID: 34951678 Free PMC article.
-
The effectiveness of patient activation intervention on type 2 diabetes mellitus glycemic control and self-management behaviors: A systematic review of RCTs.Prim Care Diabetes. 2020 Feb;14(1):12-20. doi: 10.1016/j.pcd.2019.08.009. Epub 2019 Sep 20. Prim Care Diabetes. 2020. PMID: 31543458
-
The effectiveness of patient-centered care vs. usual care in type 2 diabetes self-management: A systematic review and meta-analysis.Front Public Health. 2022 Oct 28;10:994766. doi: 10.3389/fpubh.2022.994766. eCollection 2022. Front Public Health. 2022. PMID: 36388341 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
