

Anesthetic management of a large mandibular odontogenic myxoma in a child - a case report
- PMID: 38840650
- PMCID: PMC11148415
- DOI: 10.17245/jdapm.2024.24.3.213
Anesthetic management of a large mandibular odontogenic myxoma in a child - a case report
Abstract
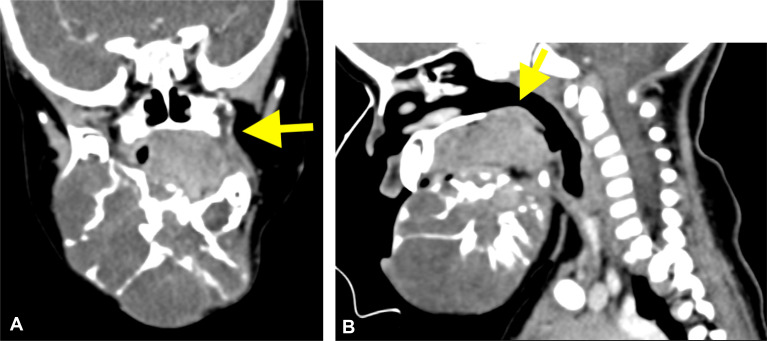
Numerous neoplastic lesions can arise in the orofacial region in the pediatric populations. Odontogenic tumors typically affect the mandible more than the maxilla. Airway management can be challenging in pediatric oral tumors because of the distorted anatomy and physiological variations. Conventional awake fiberoptic intubation is not always possible owing to limited cooperation from the pediatric populations. Herein, we report the case of a 1-year-old child with odontogenic myxoma of the mandible and an anticipated difficult airway. Given the expected difficulties in the airway, video laryngoscope-assisted orotracheal intubation under general anesthesia with maintenance of spontaneous breathing was scheduled. Proper planning and thorough examinations are vital for successful airway management in pediatric patients.
Keywords: Airway Management; Intubation; Myxoma; Odontogenic Tumors.
Copyright © 2024 Journal of Dental Anesthesia and Pain Medicine.
Conflict of interest statement
DECLARATION OF INTERESTS: None
Figures



Similar articles
-
Anesthesia management in a pediatric patient with complicatedly difficult airway: A case report.World J Clin Cases. 2023 Apr 16;11(11):2482-2488. doi: 10.12998/wjcc.v11.i11.2482. World J Clin Cases. 2023. PMID: 37123316 Free PMC article.
-
Awake Intubation for a Case of Giant Parapharyngeal Space Tumor Using McGrath MAC® Video Laryngoscope.Int Med Case Rep J. 2022 Jan 22;15:19-22. doi: 10.2147/IMCRJ.S345763. eCollection 2022. Int Med Case Rep J. 2022. PMID: 35125893 Free PMC article.
-
Maxillary and mandibular odontogenic myxomas: case report.Pan Afr Med J. 2022 Jun 8;42:103. doi: 10.11604/pamj.2022.42.103.34690. eCollection 2022. Pan Afr Med J. 2022. PMID: 36034028 Free PMC article.
-
Pediatric odontogenic fibromyxoma of the mandible: Case report and review of the literature.Head Neck. 2016 Jan;38(1):E25-8. doi: 10.1002/hed.24090. Epub 2015 Jul 18. Head Neck. 2016. PMID: 25898806 Review.
-
Surgical management of odontogenic myxoma: a case report and review of the literature.BMC Res Notes. 2014 Apr 5;7:214. doi: 10.1186/1756-0500-7-214. BMC Res Notes. 2014. PMID: 24708884 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
