

Disease Progression and Multiparametric Imaging Characteristics of Spinocerebellar Ataxia Type 3 With Spastic Paraplegia
- PMID: 38841628
- PMCID: PMC11152645
- DOI: 10.1212/NXG.0000000000200162
Disease Progression and Multiparametric Imaging Characteristics of Spinocerebellar Ataxia Type 3 With Spastic Paraplegia
Abstract
Background and objectives: Spinocerebellar ataxia type 3 (SCA3) is a hereditary ataxia that occurs worldwide. Clinical patterns were observed, including the one characterized by marked spastic paraplegia. This study investigated the clinical features, disease progression, and multiparametric imaging aspects of patients with SCA3.
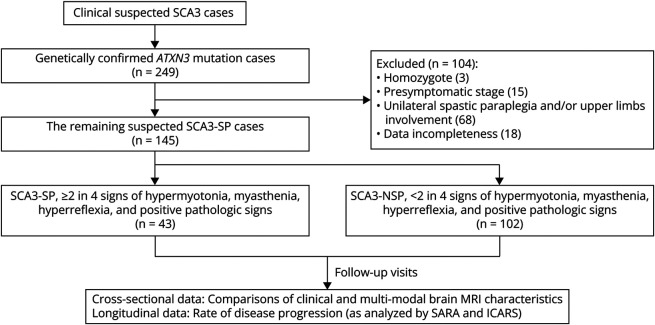
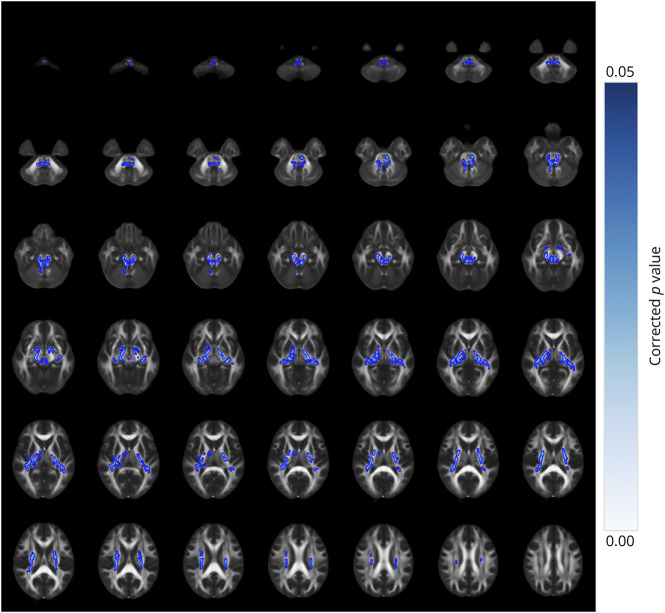
Methods: We retrospectively analyzed 249 patients with SCA3 recruited from the Organization for Southeast China for cerebellar ataxia research between October 2014 and December 2020. Of the 249 patients, 145 were selected and assigned to 2 groups based on neurologic examination: SCA3 patients with spastic paraplegia (SCA3-SP) and SCA3 patients with nonspastic paraplegia (SCA3-NSP). Participants underwent 3.0-T brain MRI examinations, and voxel-wise and volume-of-interest-based approaches were used for the resulting images. A tract-based spatial statistical approach was used to investigate the white matter (WM) alterations using diffusion tensor imaging, neurite orientation dispersion, and density imaging metrics. Multiple linear regression analyses were performed to compare the clinical and imaging parameters between the 2 groups. The longitudinal data were evaluated using a linear mixed-effects model.
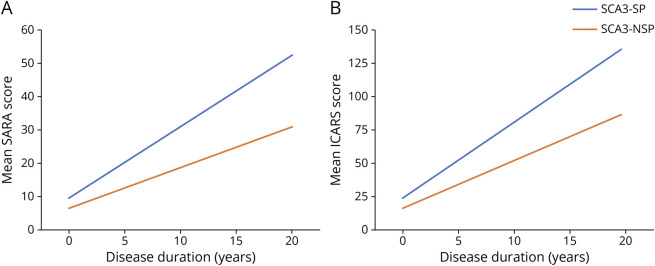
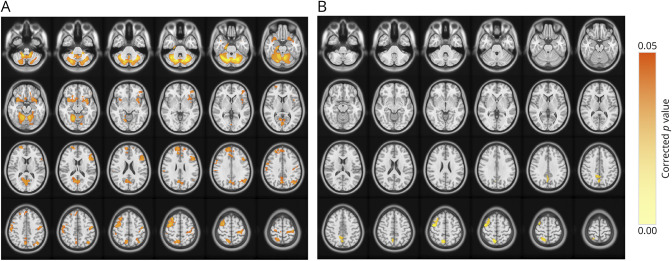
Results: Forty-three patients with SCA3-SP (mean age, 37.58years ± 11.72 [SD]; 18 women) and 102 patients with SCA3-NSP (mean age, 47.42years ± 12.50 [SD]; 39 women) were analyzed. Patients with SCA3-SP were younger and had a lower onset age but a larger cytosine-adenine-guanine repeat number, as well as higher clinical severity scores (all corrected p < 0.05). The estimated progression rates of the Scale for the Assessment and Rating of Ataxia (SARA) and International Cooperative Ataxia Rating Scale scores were higher in the SCA3-SP subgroup than in the SCA3-NSP subgroup (SARA, 2.136 vs 1.218 points; ICARS, 5.576 vs 3.480 points; both p < 0.001). In addition, patients with SCA3-SP showed gray matter volume loss in the precentral gyrus with a decreased neurite density index in the WM of the corticospinal tract and cerebellar peduncles compared with patients with SCA3-NSP.
Discussion: SCA3-SP differs from SCA3-NSP in clinical features, multiparametric brain imaging findings, and longitudinal follow-up progression.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to Neurology.org/NG for full disclosures.
Figures
References
LinkOut - more resources
Full Text Sources