

Cost effectiveness analysis of a fixed dose combination pill for primary prevention of cardiovascular disease from an individual participant data meta-analysis
- PMID: 38841710
- PMCID: PMC11152900
- DOI: 10.1016/j.eclinm.2024.102651
Cost effectiveness analysis of a fixed dose combination pill for primary prevention of cardiovascular disease from an individual participant data meta-analysis
Abstract
Background: Cardiovascular disease (CVD) continues to impart a large burden on the global population, especially in lower income countries where affordability limits the use of cardiovascular medicines. A fixed dose combination strategy of at least 2 blood pressure lowering medications and a statin with aspirin in a single pill has been shown to reduce the risk of incident CVD by 38% in primary prevention in a recent meta-analysis. We report the in-trial (median follow-up: 5 years) cost-effectiveness of a fixed dose combination (FDC) pill in different income groups based on data from that meta-analysis.
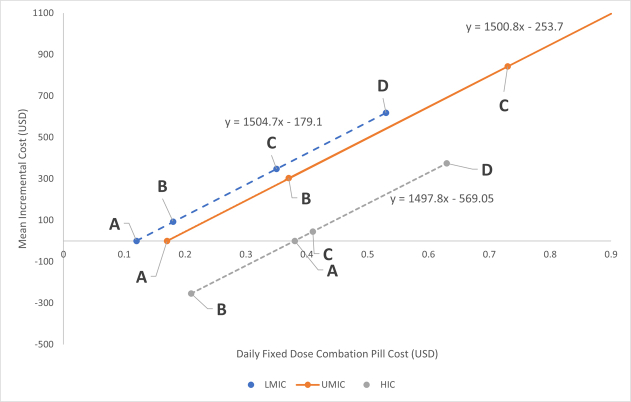
Methods: Countries were categorized using World Bank economic groups: Lower Middle Income Countries (LMIC), Upper Middle Income Countries (UMIC) and High Income Countries (HIC). Country specific costs were obtained for hospitalized events, procedures, and non-study medications (2020 USD). FDC price was based on the cheapest equivalent substitute (CES) for each component.
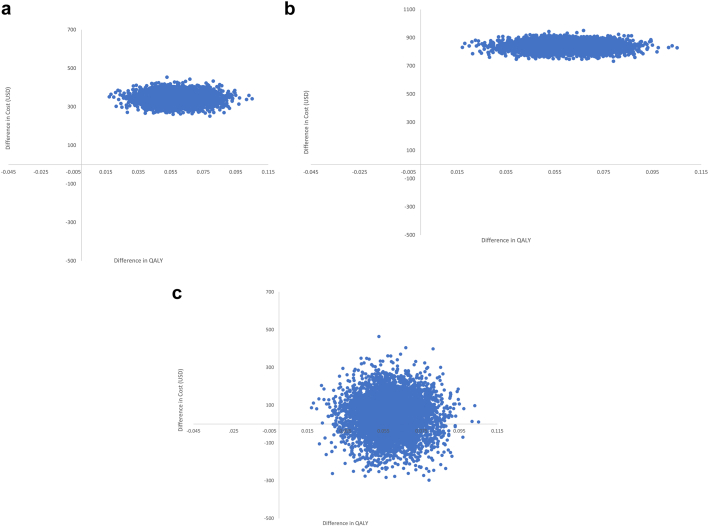
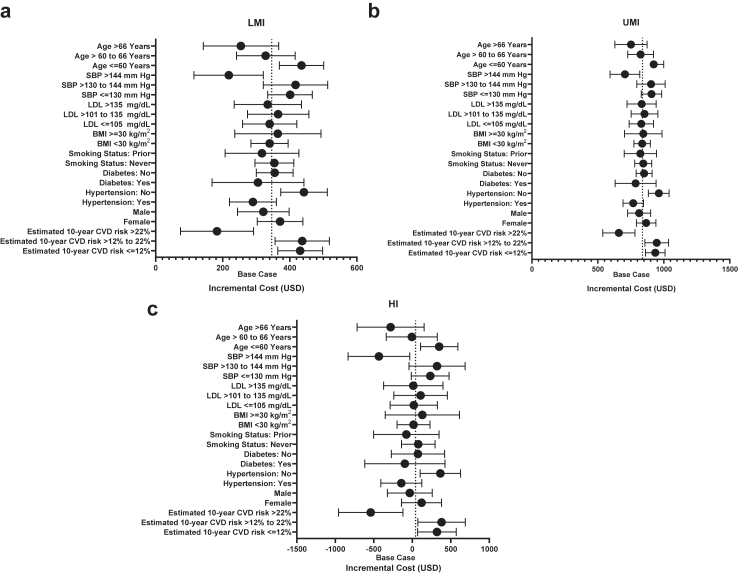
Findings: For the CES-FDC pill versus control the difference in cost was $346 (95% CI: $294-$398) per participant in Lower Middle Income Countries, $838 (95% CI: $781-$895) in Upper Middle Income Countries and $42 (95% CI: -$155 to $239) (cost-neutral) in High Income Countries. During the study period the CES-FDC pill was associated with incremental gain in quality-adjusted life years of 0.06 (95% CI: 0.04-0.08) resulting in an incremental cost-effectiveness ratio (ICER) of $5767 (95% CI: 5735-$5799), $13,937 (95% CI: $13,893-$14,041) and $700 (95% CI: $662-$738) respectively. In subgroups analyses, the highest 10 years CVD risk subgroup had ICERs of $2033, $7322 and -$6000/QALY.
Interpretation: A FDC pill produced at CES costs is cost-neutral in HIC. Governments of LMI and UMI countries should assess these results based on the ICER threshold accepted in their own country and own specific health care priorities but should consider prioritizing this strategy for patients with high 10 years CVD risk as a first step.
Funding: Population Health Research Institute.
Keywords: Cardiovascular disease; Cost implications; Cost-effectiveness; Fixed dose combination; Polypill; Primary prevention.
© 2024 The Author(s).
Conflict of interest statement
AL, WT, PJ, PG, RM, GR, PL-J, PP, AA, AD and HG have no conflicts to declare. MDH reports Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events outside the submitted work from PwC Switzerland. Support for attending meetings and/or travel outside the submitted work from the World Heart Federation. MDH has an appointment at The George Institute for Global Health, which has a patent, license, and has received investment funding with intent to commercialize fixed-dose combination therapy through its social enterprise business, George Medicines and has patents pending for Heart Failure polypills. DX reports grants from Population Health Research Institute, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Coca-Cola India, the Indian Council of Medical Research, Pfizer, UK Medical Research Council, and Wellcome Trust outside the submitted work. Speaker's fees from Eli Lilly, Sanofi and Intas outside the submitted work. Support for attending meetings and/or travel outside the submitted work from the Indian Council of Medical Research, Eli Lilly, Sanofi, BIRAC and DBC. DX is an honorary VP with SOCHARA and honorary executive committee member of ISCR. SY reports grants from AstraZeneca, and Cadila Pharmaceuticals related to conducting the HOPE-3 or TIPS-3 studies and Honoraria for lectures on the Prevention of Cardiovascular Disease from diverse sources.
Figures
Similar articles
-
The cost implications of a polypill for primary prevention in the TIPS-3 trial.Eur Heart J Qual Care Clin Outcomes. 2022 Nov 17;8(8):899-908. doi: 10.1093/ehjqcco/qcab101. Eur Heart J Qual Care Clin Outcomes. 2022. PMID: 34962984 Clinical Trial.
-
Cost-effectiveness of a fixed dose combination (polypill) in secondary prevention of cardiovascular diseases in India: Within-trial cost-effectiveness analysis of the UMPIRE trial.Int J Cardiol. 2018 Jul 1;262:71-78. doi: 10.1016/j.ijcard.2018.03.082. Epub 2018 Mar 21. Int J Cardiol. 2018. PMID: 29622506 Clinical Trial.
-
Cost-effectiveness of a fixed-dose combination pill for secondary prevention of cardiovascular disease in China, India, Mexico, Nigeria, and South Africa: a modelling study.Lancet Glob Health. 2019 Oct;7(10):e1346-e1358. doi: 10.1016/S2214-109X(19)30339-0. Epub 2019 Aug 30. Lancet Glob Health. 2019. PMID: 31477544
-
Cost-effectiveness of fixed-dose combination pill (Polypill) in primary and secondary prevention of cardiovascular disease: A systematic literature review.PLoS One. 2022 Jul 28;17(7):e0271908. doi: 10.1371/journal.pone.0271908. eCollection 2022. PLoS One. 2022. PMID: 35901100 Free PMC article.
-
Atorvastatin: a pharmacoeconomic review of its use in the primary and secondary prevention of cardiovascular events.Pharmacoeconomics. 2007;25(12):1031-53. doi: 10.2165/00019053-200725120-00005. Pharmacoeconomics. 2007. PMID: 18047388 Review.
Cited by
-
Reducing premature mortality from cardiovascular diseases in low and middle income countries: The role of Polypill in public health policy.Int J Cardiol Cardiovasc Risk Prev. 2025 Apr 3;25:200400. doi: 10.1016/j.ijcrp.2025.200400. eCollection 2025 Jun. Int J Cardiol Cardiovasc Risk Prev. 2025. PMID: 40242559 Free PMC article. Review.
References
-
- Joseph P., Leong D., McKee M., et al. Reducing the global burden of cardiovascular disease, part 1: the epidemiology and risk factors. Circ Res. 2017;121:677–694. - PubMed
-
- Anon GBD compare | IHME Viz Hub. https://vizhub.healthdata.org/gbd-compare/
-
- Yusuf S. Two decades of progress in preventing vascular disease. Lancet. 2002;360:2–3. - PubMed
LinkOut - more resources
Full Text Sources
