

Door-to-Needle Time for Extracorporeal Cardiopulmonary Resuscitation and Neurological Outcomes in Out-of-Hospital Cardiac Arrest: A Nationwide Study
- PMID: 38842281
- PMCID: PMC11255735
- DOI: 10.1161/JAHA.124.034971
Door-to-Needle Time for Extracorporeal Cardiopulmonary Resuscitation and Neurological Outcomes in Out-of-Hospital Cardiac Arrest: A Nationwide Study
Abstract
Background: Extracorporeal cardiopulmonary resuscitation (ECPR) is an option for refractory cardiac arrest, and immediate initiation after indication is recommended. However, the practical goals of ECPR preparation (such as the door-to-needle time) remain unclear. This study aimed to elucidate the association between the door-to-needle time and neurological outcomes of out-of-hospital cardiac arrest.
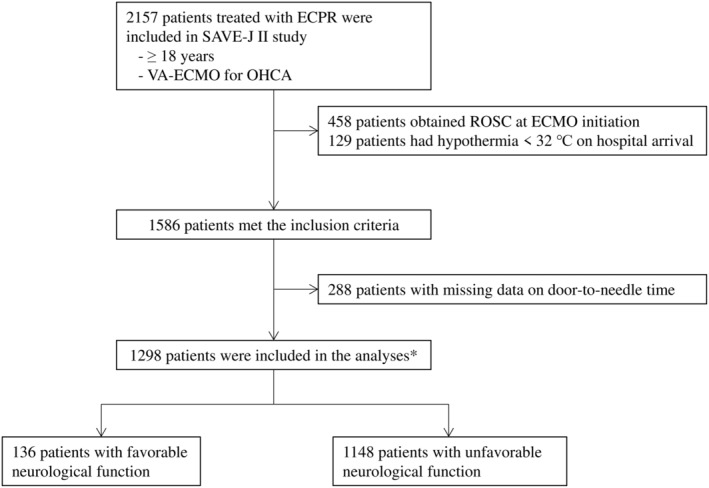
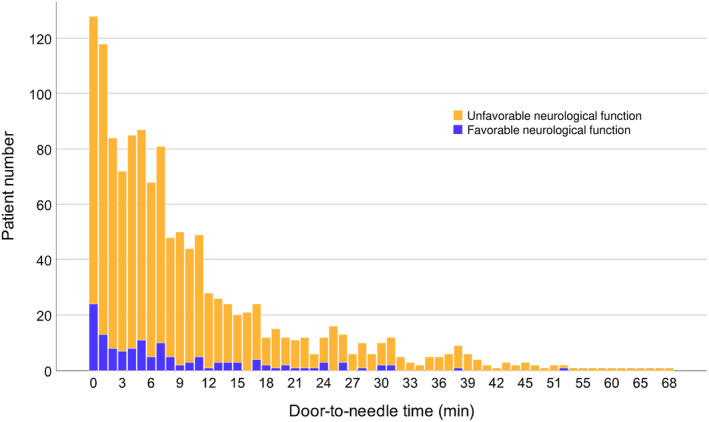
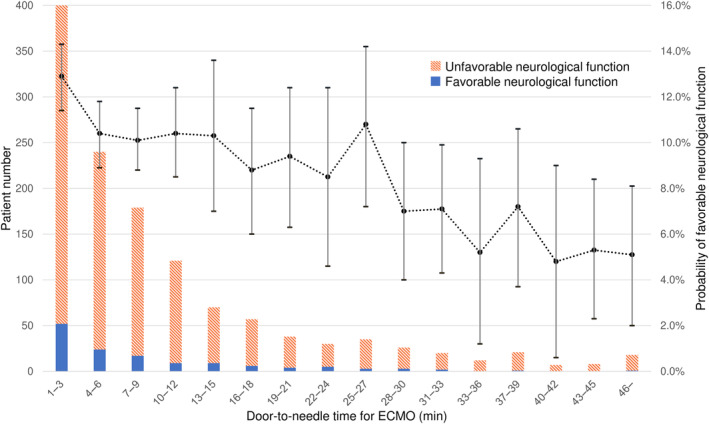
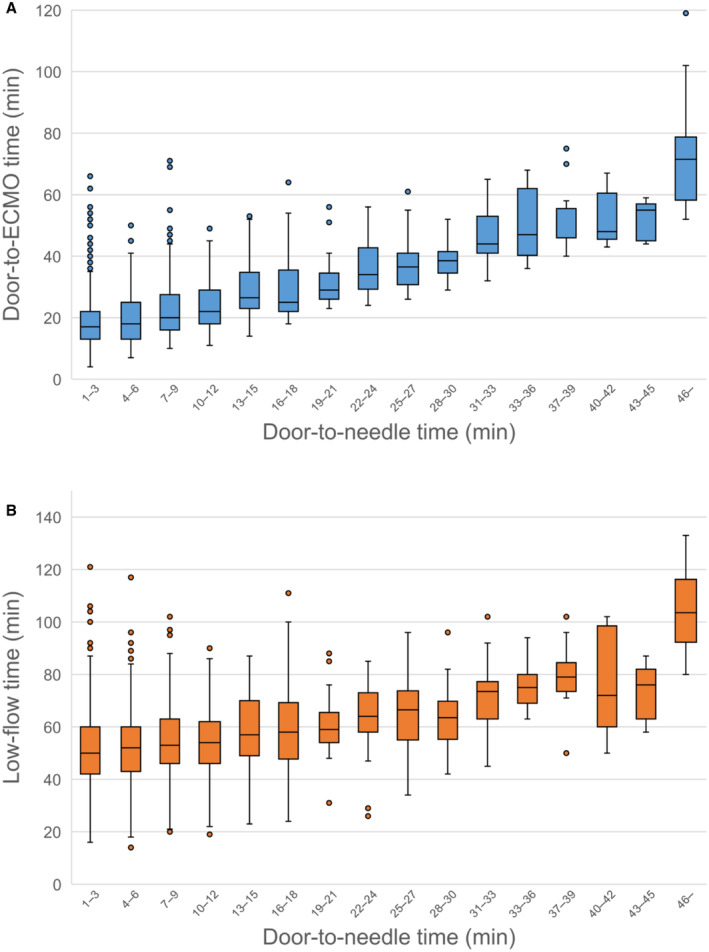
Methods and results: This is a post hoc analysis of a nationwide multicenter study on out-of-hospital cardiac arrest treated with ECPR at 36 institutions between 2013 and 2018 (SAVE-J [Study of Advanced Cardiac Life Support for Ventricular Fibrillation with Extracorporeal Circulation in Japan] II study). Adult patients without hypothermia (≥32 °C) in whom circulation was not returned at ECPR initiation were included. The probability of favorable neurological function at 30 days (defined as Cerebral Performance Category ≤2) was estimated using a generalized estimating equations model, in which institutional, patient, and treatment characteristics were adjusted. Estimated probabilities were then calculated according to the door-to-needle time with 3-minute increments, and a clinical threshold was assumed. Among 1298 patients eligible for this study, 136 (10.6%) had favorable neurological function. The estimated probability of favorable outcomes was highest in patients with 1 to 3 minutes of door-to-needle time (12.9% [11.4%-14.3%]) and remained at 9% to 10% until 27 to 30 minutes. Then, the probability dropped gradually with each 3-minute delay. A 30-minute threshold was assumed, and shorter door-to-extracorporeal membrane oxygenation/low-flow time and fewer adverse events related to cannulation were observed in patients with door-to-needle time <30 minutes.
Conclusions: The probability of favorable functions after out-of-hospital cardiac arrest decreased as the door-to-needle time for ECPR was prolonged, with a rapid decline after 27 to 30 minutes.
Registration: URL: https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000041577; Unique identifier: UMIN000036490.
Keywords: Cerebral Performance Category; cardiopulmonary resuscitation; extracorporeal cardiopulmonary resuscitation.
Figures
References
-
- Goto Y, Funada A, Goto Y. Relationship between the duration of cardiopulmonary resuscitation and favorable neurological outcomes after out‐of‐hospital cardiac arrest: a prospective, Nationwide, population‐based cohort study. J Am Heart Assoc. 2016;5:e002819. doi: 10.1161/JAHA.115.002819 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
