

Home Blood Pressure Telemonitoring and Nurse Case Management in Black and Hispanic Patients With Stroke: A Randomized Clinical Trial
- PMID: 38842799
- PMCID: PMC11157441
- DOI: 10.1001/jama.2024.6609
Home Blood Pressure Telemonitoring and Nurse Case Management in Black and Hispanic Patients With Stroke: A Randomized Clinical Trial
Abstract
Importance: Black and Hispanic patients have high rates of recurrent stroke and uncontrolled hypertension in the US. The effectiveness of home blood pressure telemonitoring (HBPTM) and telephonic nurse case management (NCM) among low-income Black and Hispanic patients with stroke is unknown.
Objective: To determine whether NCM plus HBPTM results in greater systolic blood pressure (SBP) reduction at 12 months and lower rate of stroke recurrence at 24 months than HBPTM alone among Black and Hispanic stroke survivors with uncontrolled hypertension.
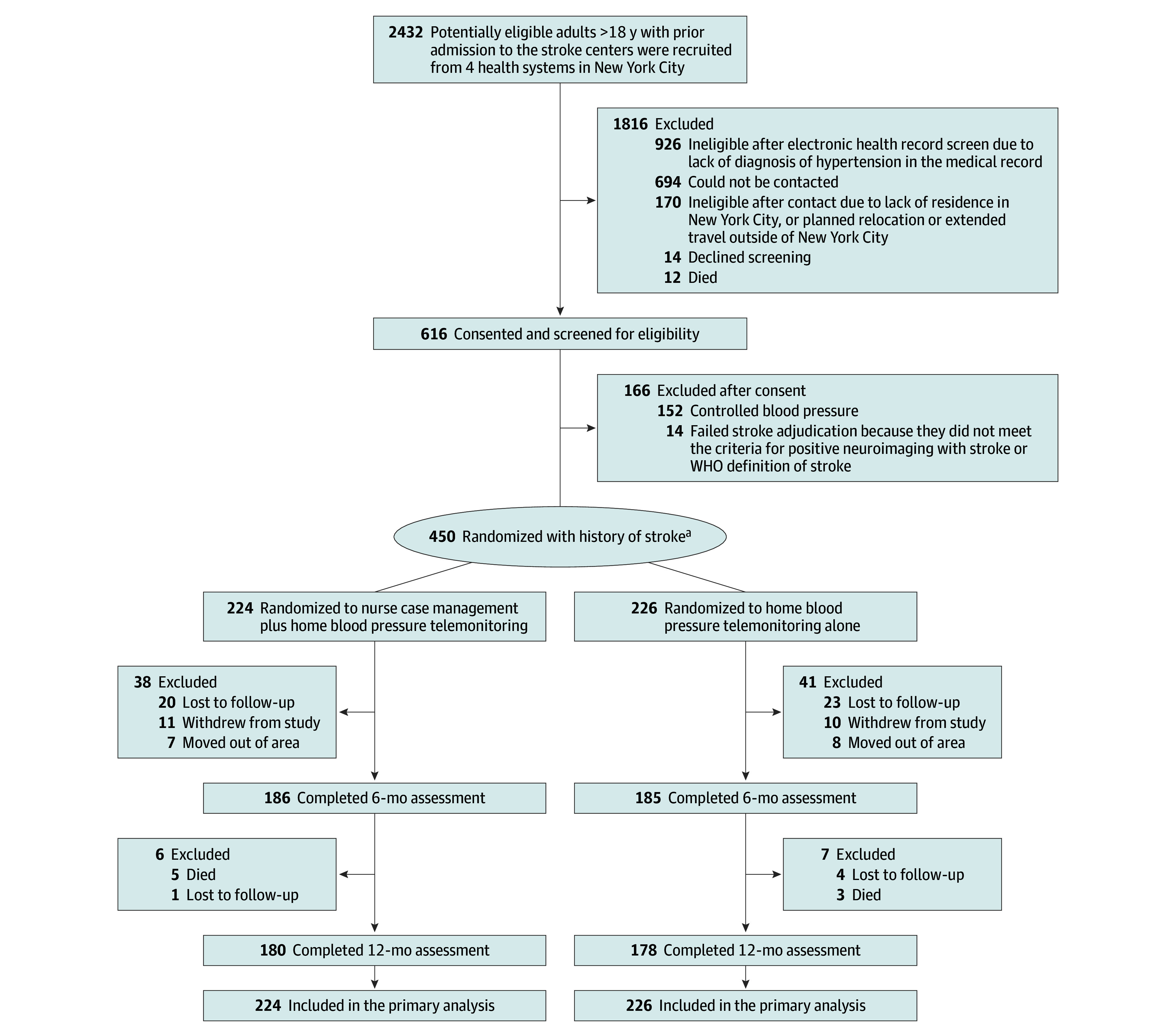
Design, setting, and participants: Practice-based, multicenter, randomized clinical trial in 8 stroke centers and ambulatory practices in New York City. Black and Hispanic study participants were enrolled between April 18, 2014, and December 19, 2017, with a final follow-up visit on December 31, 2019.
Interventions: Participants were randomly assigned to receive either HBPTM alone (12 home BP measurements/week for 12 months, with results transmitted to a clinician; n = 226) or NCM plus HBPTM (20 counseling calls over 12 months; n = 224).
Main outcomes and measures: Primary outcomes were change in SBP at 12 months and rate of recurrent stroke at 24 months. Final statistical analyses were completed March 14, 2024.
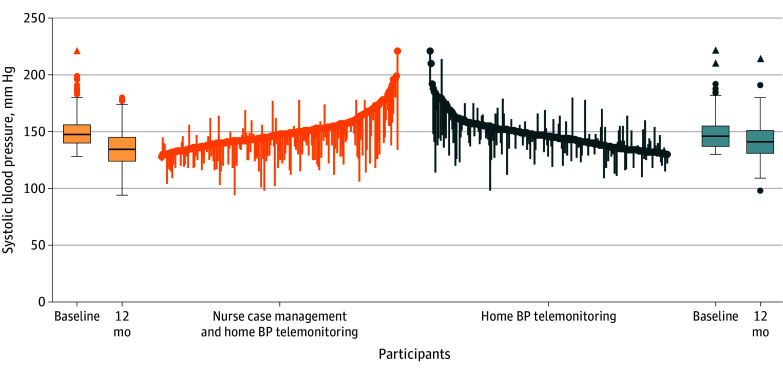
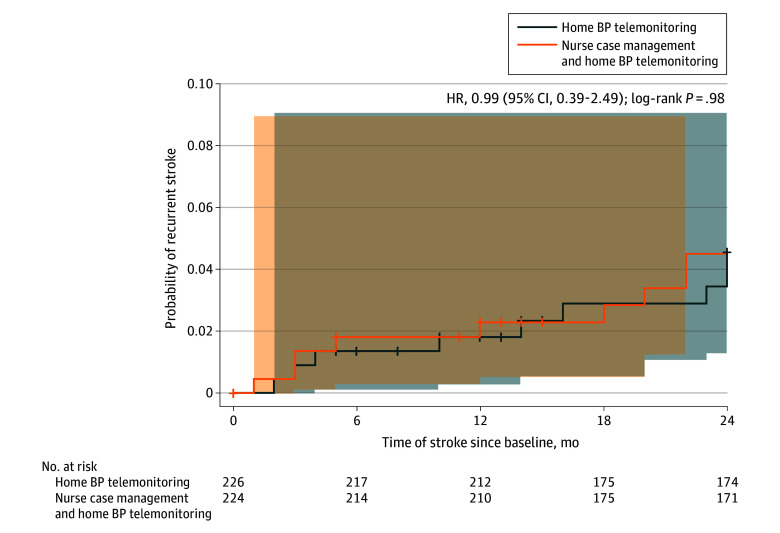
Results: Among 450 participants who were enrolled and randomized (mean [SD] age, 61.7 [11.0] years; 51% were Black [n = 231]; 44% were women [n = 200]; 31% had ≥3 comorbid conditions [n = 137]; 72% had household income <$25 000/y [n = 234/324]), 358 (80%) completed the trial. Those in the NCM plus HBPTM group had a significantly greater SBP reduction than those in the HBPTM alone group at 12 months (-15.1 mm Hg [95% CI, -17.2 to -13.0] vs -5.8 mm Hg [95% CI, -7.9 to -3.7], respectively; P < .001). The between-group difference in SBP reduction at 12 months, adjusted for primary care physician clustering, was -8.1 mm Hg (95% CI, -11.2 to -5.0; P < .001) at 12 months. The rate of recurrent stroke was similar between both groups at 24 months (4.0% in the NCM plus HBPTM group vs 4.0% in the HBPTM alone group, P > .99).
Conclusions and relevance: Among predominantly low-income Black and Hispanic stroke survivors with uncontrolled hypertension, addition of NCM to HBPTM led to greater SBP reduction than HBPTM alone. Additional studies are needed to understand the long-term clinical outcomes, cost-effectiveness, and generalizability of NCM-enhanced telehealth programs among low-income Black and Hispanic stroke survivors with significant comorbidity.
Trial registration: Clinical Trials.gov Identifier: NCT02011685.
Conflict of interest statement
Figures
References
-
- Lackland DT, Roccella EJ, Deutsch AF, et al. ; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; Council on Functional Genomics and Translational Biology . Factors influencing the decline in stroke mortality: a statement from the American Heart Association/American Stroke Association. Stroke. 2014;45(1):315-353. doi: 10.1161/01.str.0000437068.30550.cf - DOI - PMC - PubMed
-
- O’Donnell MJ, Chin SL, Rangarajan S, et al. ; INTERSTROKE investigators . Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761-775. doi: 10.1016/S0140-6736(16)30506-2 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
