

"Long-term effects of center volume on transplant outcomes in adult kidney transplant recipients"
- PMID: 38843258
- PMCID: PMC11156332
- DOI: 10.1371/journal.pone.0301425
"Long-term effects of center volume on transplant outcomes in adult kidney transplant recipients"
Abstract
Background: The influence of center volume on kidney transplant outcomes is a topic of ongoing debate. In this study, we employed competing risk analyses to accurately estimate the marginal probability of graft failure in the presence of competing events, such as mortality from other causes with long-term outcomes. The incorporation of immunosuppression protocols and extended follow-up offers additional insights. Our emphasis on long-term follow-up aligns with biological considerations where competing risks play a significant role.
Methods: We examined data from 219,878 adult kidney-only transplantations across 256 U.S. transplant centers (January 2001-December 2015) sourced from the Organ Procurement and Transplantation Network registry. Centers were classified into quartiles by annual volume: low (Q1 = 28), medium (Q2 = 75), medium-high (Q3 = 121), and high (Q4 = 195). Our study investigated the relationship between center volume and 5-year outcomes, focusing on graft failure and mortality. Sub-population analyses included deceased donors, living donors, diabetic recipients, those with kidney donor profile index >85%, and re-transplants from deceased donors.
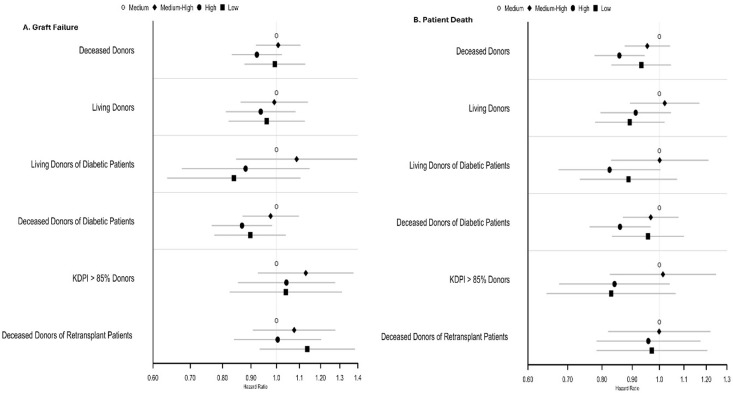
Results: Adjusted cause-specific hazard ratios (aCHR) for Five-Year Graft Failure and Patient Death were examined by center volume, with low-volume centers as the reference standard (aCHR: 1.0). In deceased donors, medium-high and high-volume centers showed significantly lower cause-specific hazard ratios for graft failure (medium-high aCHR = 0.892, p<0.001; high aCHR = 0.953, p = 0.149) and patient death (medium-high aCHR = 0.828, p<0.001; high aCHR = 0.898, p = 0.003). Among living donors, no significant differences were found for graft failure, while a trend towards lower cause-specific hazard ratios for patient death was observed in medium-high (aCHR = 0.895, p = 0.107) and high-volume centers (aCHR = 0.88, p = 0.061).
Conclusion: Higher center volume is associated with significantly lower cause-specific hazard ratios for graft failure and patient death in deceased donors, while a trend towards reduced cause-specific hazard ratios for patient death is observed in living donors.
Copyright: © 2024 Azhar et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare on conflict of interest related to this work. G Gupta has received honoraria from Alexion, CareDx, Mallinckrodt; has served on the Scientific Advisory Board for CareDx, Natera, Relypsa, Veloxis; and has received research funding from Gilead and Merck.
Figures

Similar articles
-
Association of Kidney Transplant Center Volume With 3-Year Clinical Outcomes.Am J Kidney Dis. 2019 Oct;74(4):441-451. doi: 10.1053/j.ajkd.2019.02.019. Epub 2019 May 7. Am J Kidney Dis. 2019. PMID: 31076173 Free PMC article.
-
Better kidney allograft survival despite higher-risk donor and recipient characteristics between 1995 and 2014.Nephrol Dial Transplant. 2024 Oct 30;39(11):1846-1855. doi: 10.1093/ndt/gfae081. Nephrol Dial Transplant. 2024. PMID: 38573827 Free PMC article.
-
Association of Deceased Donor Acute Kidney Injury With Recipient Graft Survival.JAMA Netw Open. 2020 Jan 3;3(1):e1918634. doi: 10.1001/jamanetworkopen.2019.18634. JAMA Netw Open. 2020. PMID: 31913491 Free PMC article.
-
An Integrative Review of Frailty, Patient Mortality and Graft Failure in Solid Organ Transplant.Prog Transplant. 2025 Jun;35(2):97-109. doi: 10.1177/15269248251343387. Epub 2025 May 19. Prog Transplant. 2025. PMID: 40388942 Review.
-
Competing Risks Analysis of Kidney Transplant Waitlist Outcomes: Two Important Statistical Perspectives.Kidney Int Rep. 2024 Feb 1;9(6):1580-1589. doi: 10.1016/j.ekir.2024.01.050. eCollection 2024 Jun. Kidney Int Rep. 2024. PMID: 38899174 Free PMC article. Review.
References
-
- Tsampalieros A., Knoll G. A., Fergusson N., Bennett A., Taljaard M., and Fergusson D., “Center Variation and the Effect of Center and Provider Characteristics on Clinical Outcomes in Kidney Transplantation: A Systematic Review of the Evidence,” Can. J. Kidney Health Dis., vol. 4, p. 2054358117735523, Oct. 2017, doi: 10.1177/2054358117735523 - DOI - PMC - PubMed
-
- Axelrod D. A., Guidinger M. K., McCullough K. P., Leichtman A. B., Punch J. D., and Merion R. M., “Association of center volume with outcome after liver and kidney transplantation,” Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg., vol. 4, no. 6, pp. 920–927, Jun. 2004, doi: 10.1111/j.1600-6143.2004.00462.x - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
