

Myocardial Inflammation in Heart Failure With Reduced and Preserved Ejection Fraction
- PMID: 38843295
- PMCID: PMC11160997
- DOI: 10.1161/CIRCRESAHA.124.323659
Myocardial Inflammation in Heart Failure With Reduced and Preserved Ejection Fraction
Abstract
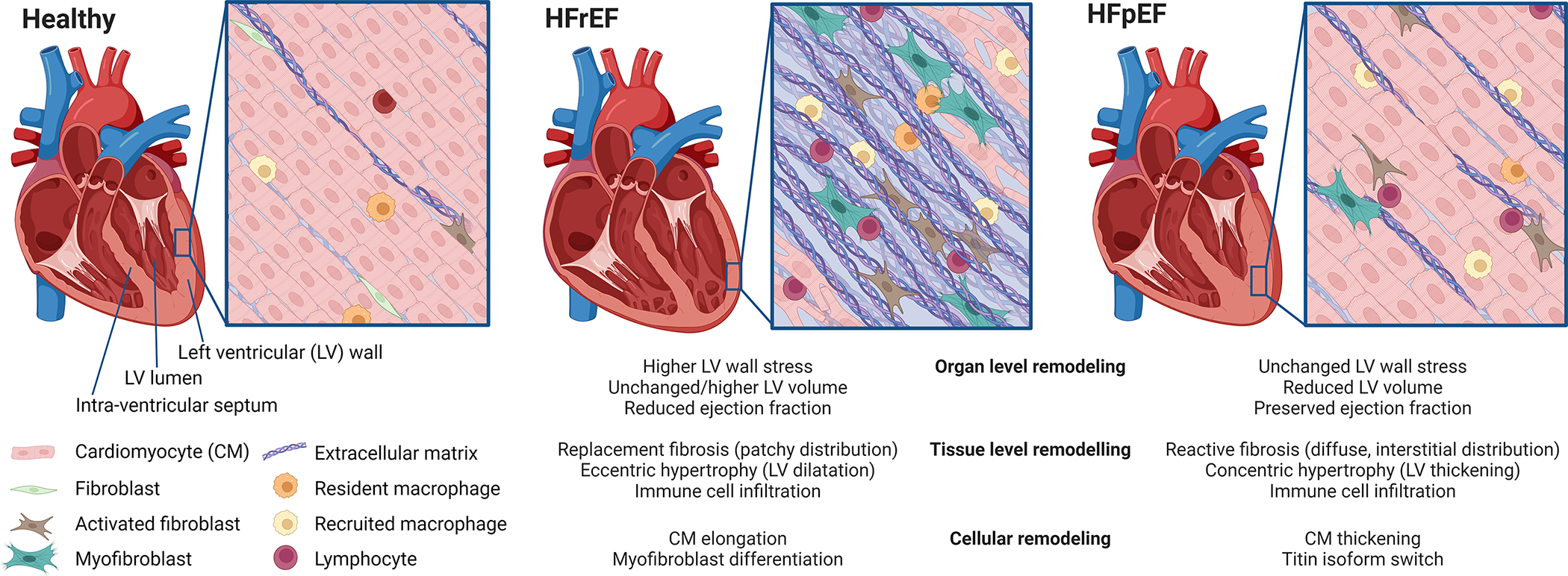
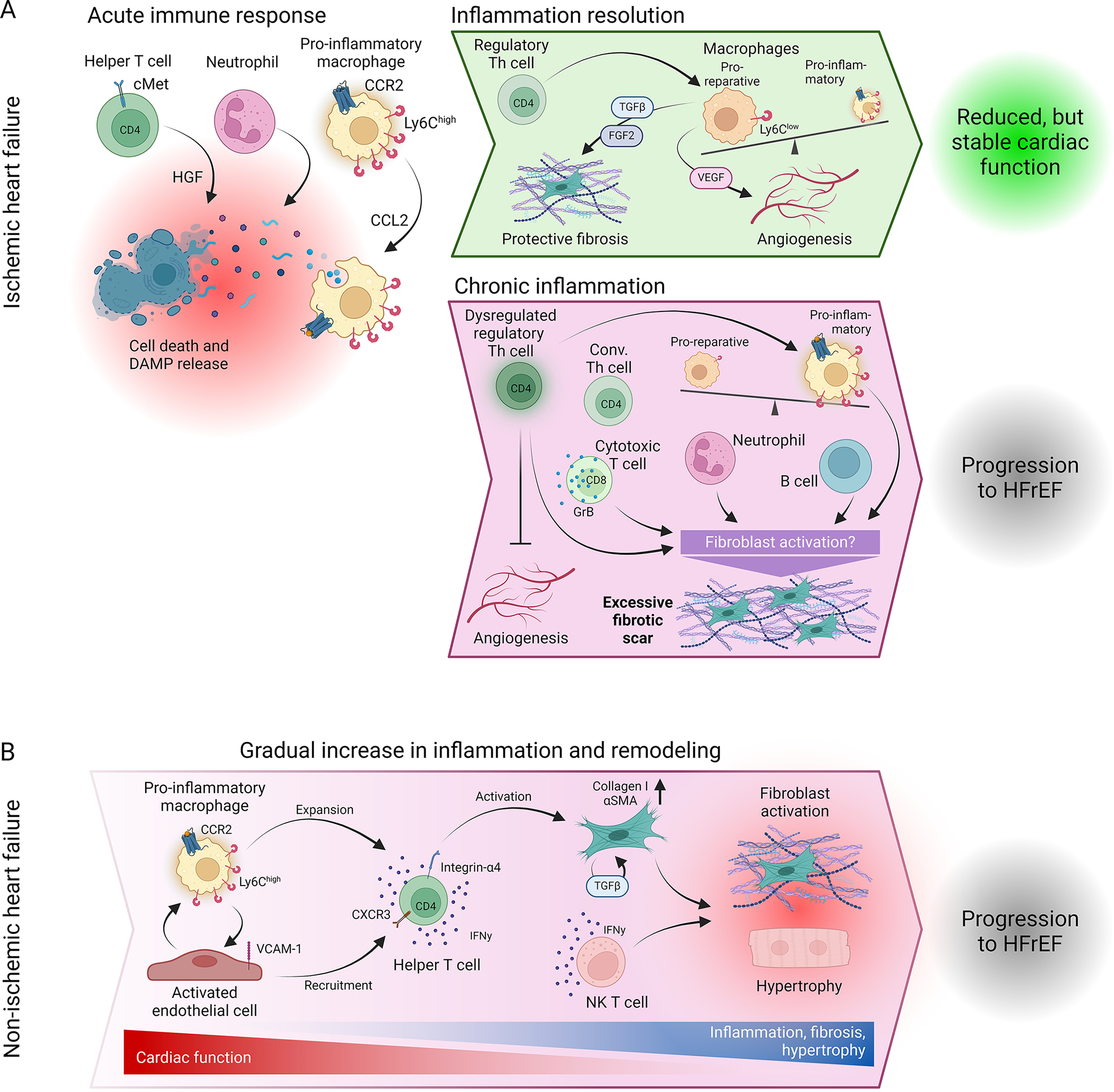
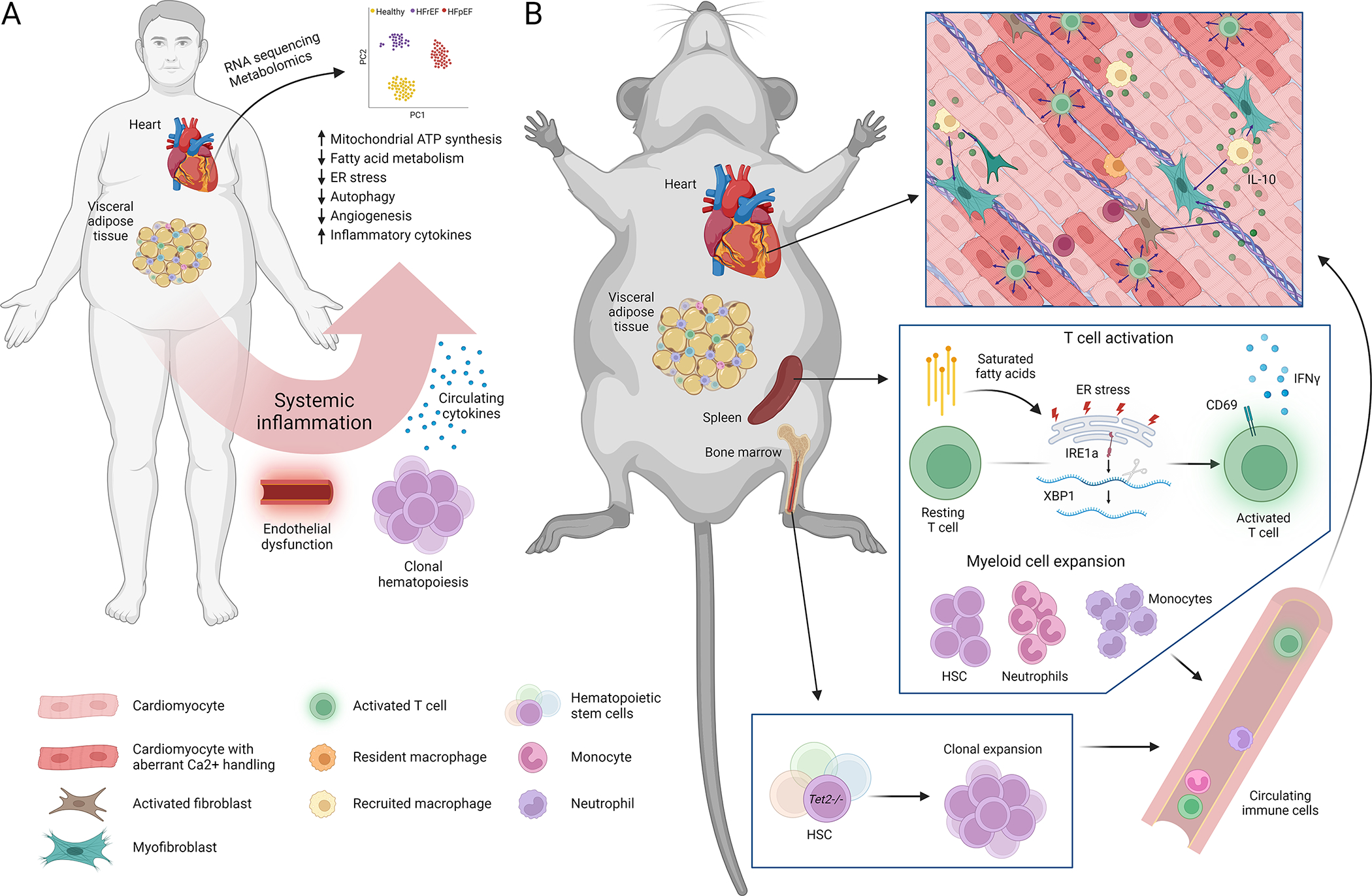
Heart failure (HF) is characterized by a progressive decline in cardiac function and represents one of the largest health burdens worldwide. Clinically, 2 major types of HF are distinguished based on the left ventricular ejection fraction (EF): HF with reduced EF and HF with preserved EF. While both types share several risk factors and features of adverse cardiac remodeling, unique hallmarks beyond ejection fraction that distinguish these etiologies also exist. These differences may explain the fact that approved therapies for HF with reduced EF are largely ineffective in patients suffering from HF with preserved EF. Improving our understanding of the distinct cellular and molecular mechanisms is crucial for the development of better treatment strategies. This article reviews the knowledge of the immunologic mechanisms underlying HF with reduced and preserved EF and discusses how the different immune profiles elicited may identify attractive therapeutic targets for these conditions. We review the literature on the reported mechanisms of adverse cardiac remodeling in HF with reduced and preserved EF, as well as the immune mechanisms involved. We discuss how the knowledge gained from preclinical models of the complex syndrome of HF as well as from clinical data obtained from patients may translate to a better understanding of HF and result in specific treatments for these conditions in humans.
Keywords: heart failure; immune system; inflammation; ventricular function, left; ventricular remodeling.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
