

Theta burst stimulation for depression: a systematic review and network and pairwise meta-analysis
- PMID: 38844532
- PMCID: PMC11609094
- DOI: 10.1038/s41380-024-02630-5
Theta burst stimulation for depression: a systematic review and network and pairwise meta-analysis
Abstract
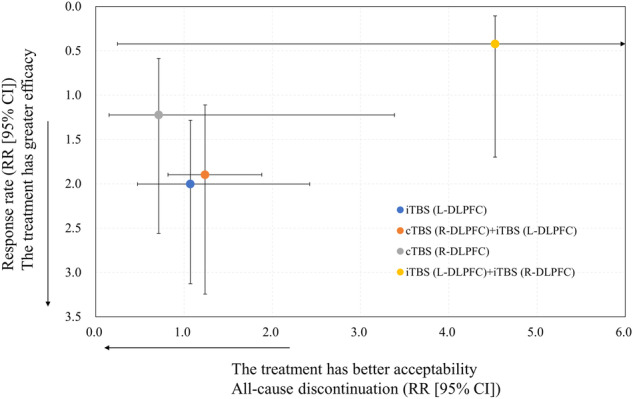
In clinical practice, theta burst stimulation (TBS) presents as a more efficient and potentially more effective therapeutic modality than conventional repetitive transcranial magnetic stimulation (rTMS), as it allows for the delivery of more stimuli in less time and at similar intensities. To date, accelerated treatment plans according to various continuous (cTBS) and intermittent TBS (iTBS) protocols for depression have been proposed. To investigate which of the TBS protocols provided a favorable risk-benefit balance for individuals with depression, this systematic review and random-effects model network meta-analysis was conducted. The study outcomes included response rate (primary), depression symptom improvement, remission rate, all-cause discontinuation rate, incidence of switch to mania, and incidence of headache/discomfort at treatment site. In this meta-analysis, a total of 23 randomized controlled trials (n = 960, mean age = 41.88 years, with 60.78% females) were included. Approximately 69.57% of the trials included individuals with an exclusive diagnosis of major depressive disorder. The following six TBS protocols (target) were evaluated: cTBS (right-dorsolateral prefrontal cortex [R-DLPFC]), cTBS (R-DLPFC) + iTBS (left-DLPFC [L-DLPFC]), iTBS (L-DLPFC), iTBS (L-DLPFC) + iTBS (R-DLPFC), iTBS (left-dorsomedial prefrontal cortex) + iTBS (right-dorsomedial prefrontal cortex), and iTBS (occipital lobe). Compared to sham, cTBS (R-DLPFC) + iTBS (L-DLPFC), iTBS (L-DLPFC), and iTBS (occipital lobe) had a higher response rate (k = 23); cTBS (R-DLPFC) + iTBS (L-DLPFC) and iTBS (L-DLPFC) dominated in the depression symptom improvement (k = 23); and iTBS (L-DLPFC) had a higher remission rate (k = 15). No significant differences were found for all-cause discontinuation rate (k = 17), incidence of switch to mania (k = 7), and incidence of headache/discomfort at treatment site (k = 10) between any TBS protocols and sham. Thus, cTBS (R-DLPFC) + iTBS (L-DLPFC) and iTBS (L-DLPFC) demonstrate favorable risk-benefit balance for the treatment of depression.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: All authors have no conflicts of interest to declare concerning this study. They also declare any potential competing interests that have arisen in the last 3 years. Dr. Kishi has received speaker’s honoraria from Eisai, Janssen, Meiji, Otsuka, Sumitomo, Takeda, Mitsubishi-Tanabe, Kyowa, Yoshitomi, and Viatris and research grants from Eisai, JSPS KAKENHI (19K08082 and 23K06998), Japan Agency for Medical Research and Development (JP22dk0307107, JP22wm0525024, JP23dk0307122, and 24dk0307129), and the Japanese Ministry of Health, Labor and Welfare (21GC1018). Dr. Ikuta has nothing to disclose. Dr. Sakuma has received speaker’s honoraria from daiichisankyo, Eisai, Janssen, Kyowa, Meiji, Otsuka, Sumitomo, and Takeda and has received a Fujita Health University School of Medicine Research Grant for Early-Career Scientists, Grant-in-Aid for Young Scientists (B)(19K17099), Grant-in-Aid for Scientific Research (C)(23K06998), and Japan Agency for Medical Research and Development (JP22dk0307107 and JP23dk0307122). Dr. Hatano received the speaker’s honoraria from Meiji and Sumitomo, and has received Grant-in-Aid for Early-Career Scientists (23K14827). Dr. Matsuda has received the speaker’s honoraria from Janssen, Lundbeck, Sumitomo, Otsuka, Takeda, Teijin, and Viatris, and a research grant from the Japan Agency for Medical Research and Development (24dk0307126). Mr. Wilkening was supported by the Göttingen Promotionskolleg für Medizinstudierende, funded by the Jacob-Henle-Programm/Else-Kröner-Fresenius-Stiftung. Dr. Goya-Maldonado declares no conflict of interest. His work was supported by the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung, BMBF: 01 ZX 1507, “PreNeSt - e:Med”). Dr. Tik has nothing to disclose. Dr. Williams is a named inventor on Stanford-owned intellectual property relating to accelerated TMS pulse pattern sequences and neuroimaging-based TMS targeting; he has served on scientific advisory boards for Otsuka, NeuraWell, Nooma, and Halo Neuroscience; and he has equity/stock options in Magnus Medical, NeuraWell, and Nooma. Dr. Kito received speaker honoraria from Inter Reha, Lundbeck, Sumitomo, Otsuka, Takeda, Teijin, and Viatris, consultant fees from Teijin, and research grants from Teijin. Dr. Iwata has received speaker’s honoraria from Eisai, Janssen, Meiji, Otsuka, Sumitomo, Takeda, Mitsubishi-Tanabe, and Viatris and research grants from Daiichi Sankyo, Eisai, Meiji, Otsuka, Sumitomo, Takeda, Tanabe-Mitsubishi, Grant-in-Aid for Scientific Research (B)(22H03003), and Japan Agency for Medical Research and Development (JP22wm0425008).
Figures

References
-
- Milev RV, Giacobbe P, Kennedy SH, Blumberger DM, Daskalakis ZJ, Downar J, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 4. Neurostimulation treatments. Can J Psychiatry. 2016;61:561–75. - PMC - PubMed
-
- Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin Neurophysiol. 2015;126:1071–107. - PMC - PubMed
-
- Fitzgerald PB. Targeting repetitive transcranial magnetic stimulation in depression: do we really know what we are stimulating and how best to do it? Brain Stimul. 2021;14:730–6. - PubMed
-
- Tik M, Woletz M, Schuler AL, Vasileiadi M, Cash RFH, Zalesky A, et al. Acute TMS/fMRI response explains offline TMS network effects - An interleaved TMS-fMRI study. Neuroimage. 2023;267:119833. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
