

Predicting short-term outcomes in brain-injured patients: a comprehensive approach with transcranial Doppler and intracranial compliance assessment
- PMID: 38844603
- PMCID: PMC11604736
- DOI: 10.1007/s10877-024-01181-y
Predicting short-term outcomes in brain-injured patients: a comprehensive approach with transcranial Doppler and intracranial compliance assessment
Abstract
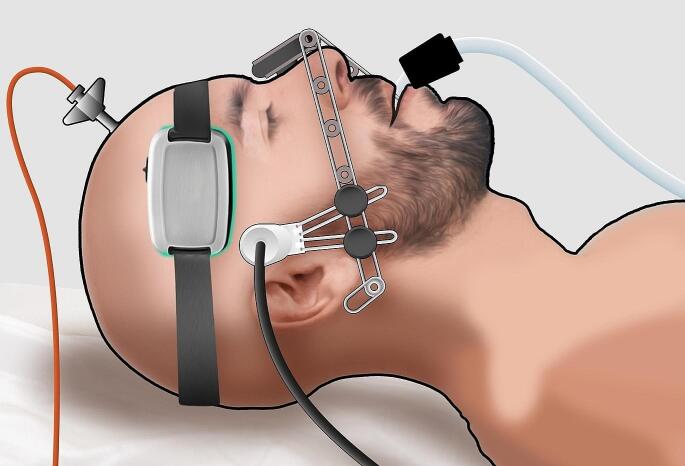
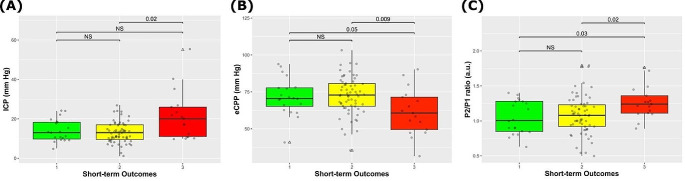
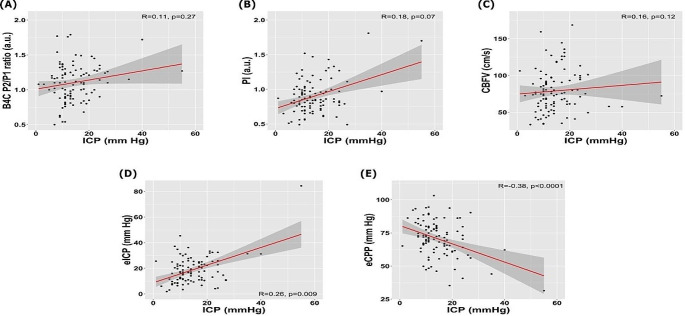
Neurocritical patients frequently exhibit abnormalities in cerebral hemodynamics (CH) and/or intracranial compliance (ICC), all of which significantly impact their clinical outcomes. Transcranial Doppler (TCD) and the cranial micro-deformation sensor (B4C) are valuable techniques for assessing CH and ICC, respectively. However, there is a scarcity of data regarding the predictive value of these techniques in determining patient outcomes. We prospectively included neurocritical patients undergoing intracranial pressure (ICP) monitoring within the first 5 days of hospital admission for TCD and B4C assessments. Comprehensive clinical data were collected alongside parameters obtained from TCD (including the estimated ICP [eICP] and estimated cerebral perfusion pressure [eCPP]) and B4C (measured as the P2/P1 ratio). These parameters were evaluated individually as well as in combination. The short-term outcomes (STO) of interest were the therapy intensity levels (TIL) for ICP management recommended by the Seattle International Brain Injury Consensus Conference, as TIL 0 (STO 1), TIL 1-3 (STO 2) and death (STO 3), at the seventh day after last data collection. The dataset was randomly separated in test and training samples, area under the curve (AUC) was used to represent the noninvasive techniques ability on the STO prediction and association with ICP. A total of 98 patients were included, with 67% having experienced severe traumatic brain injury and 15% subarachnoid hemorrhage, whilst the remaining patients had ischemic or hemorrhagic stroke. ICP, P2/P1, and eCPP demonstrated the highest ability to predict early mortality (p = 0.02, p = 0.02, and p = 0.006, respectively). P2/P1 was the only parameter significant for the prediction of STO 1 (p = 0.03). Combining B4C and TCD parameters, the highest AUC was 0.85 to predict death (STO 3), using P2/P1 + eCPP, whereas AUC was 0.72 to identify ICP > 20 mmHg using P2/P1 + eICP. The combined noninvasive neuromonitoring approach using eCPP and P2/P1 ratio demonstrated improved performance in predicting outcomes during the early phase after acute brain injury. The correlation with intracranial hypertension was moderate, by means of eICP and P2/P1 ratio. These results support the need for interpretation of this information in the ICU and warrant further investigations for the definition of therapy strategies using ancillary tests.
Keywords: Acute brain injury; Cerebral hemodynamics; Intracranial compliance; Intracranial pressure; Transcranial Doppler; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical statement: The manuscript complies with all instructions to authors. Authorship requirements have been met and the final manuscript was approved by all authors giving consent for its publication. This manuscript has not been published elsewhere and is not under consideration by another journal. The authors confirm adherence to ethical guidelines and approvals (IRB/CAAE: 66721217.0.0000.0068 by the University of São Paulo School of Medicine Ethics Committee). Checklist for diagnostic accuracy studies (STARD) was applied (supplemental). The present manuscript has a previous version posted online before peer review (preprint), available at https://www.researchsquare.com/article/rs-3406169/v1 . Competing interests: Sérgio Brasil and Danilo Cardim have recently joined brain4care’s scientific committee. The other authors declare no competing interests.
Figures
References
-
- Lahiri S, Mayer SA, Fink ME, et al. Mechanical ventilation for acute stroke: a multi-state population-based study. Neurocrit Care. 2015;23(1):28–32. - PubMed
-
- Martin NA, Patwardhan RV, Alexander MJ, et al. Characterization of cerebral hemodynamic phases following severe head trauma: hypoperfusion, hyperemia, and vasospasm. J Neurosurg. 1997;87(1):9–19. - PubMed
-
- Mataczynski C, Kazimierska A, Uryga A. Intracranial pressure pulse morphology-based definition of life-threatening intracranial hypertension episodes. Annu Int Conf IEEE Eng Med Biol Soc. 2022;2022:1742–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
