

Role of cardiac magnetic resonance in stratifying arrhythmogenic risk in mitral valve prolapse patients: a systematic review and meta-analysis
- PMID: 38844620
- PMCID: PMC11519141
- DOI: 10.1007/s00330-024-10815-3
Role of cardiac magnetic resonance in stratifying arrhythmogenic risk in mitral valve prolapse patients: a systematic review and meta-analysis
Abstract
Objectives: To perform a systematic review and meta-analysis of studies investigating the diagnostic value of cardiac magnetic resonance (CMR) features for arrhythmic risk stratification in mitral valve prolapse (MVP) patients.
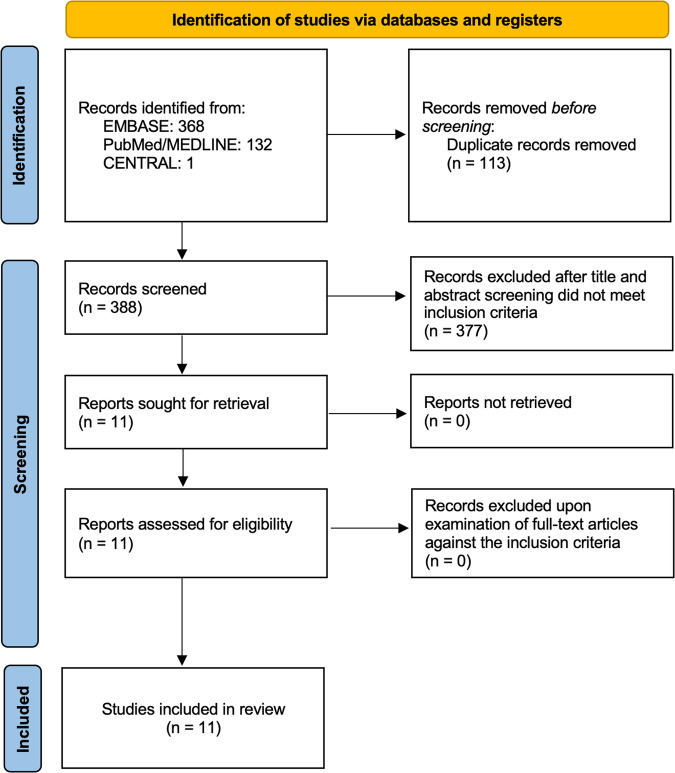
Materials and methods: EMBASE, PubMed/MEDLINE, and CENTRAL were searched for studies reporting MVP patients who underwent CMR with assessment of: left ventricular (LV) size and function, mitral regurgitation (MR), prolapse distance, mitral annular disjunction (MAD), curling, late gadolinium enhancement (LGE), and T1 mapping, and reported the association with arrhythmia. The primary endpoint was complex ventricular arrhythmias (co-VAs) as defined by any non-sustained ventricular tachycardia, sustained ventricular tachycardia, ventricular fibrillation, or aborted sudden cardiac death. Meta-analysis was performed when at least three studies investigated a CMR feature. PROSPERO registration number: CRD42023374185.
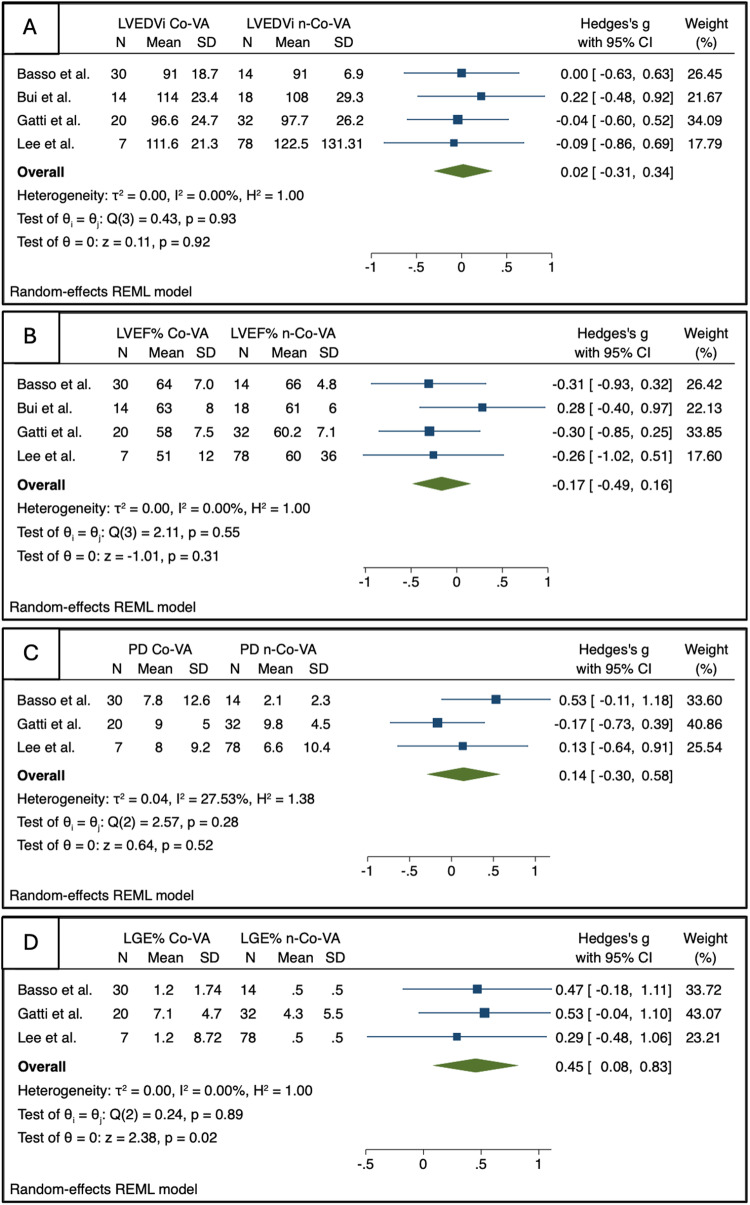
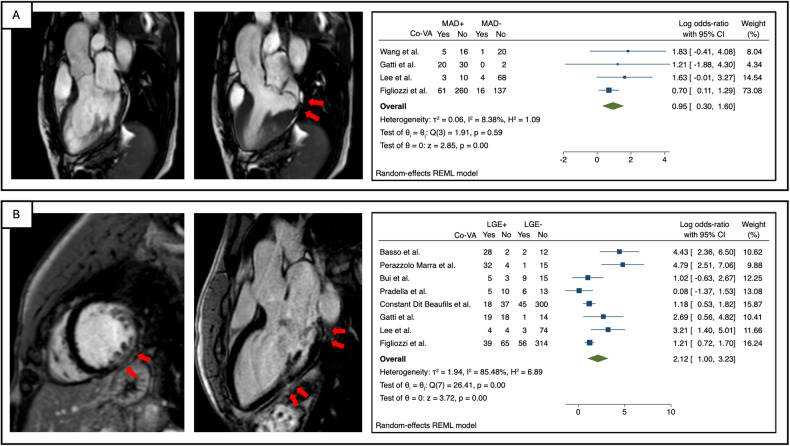
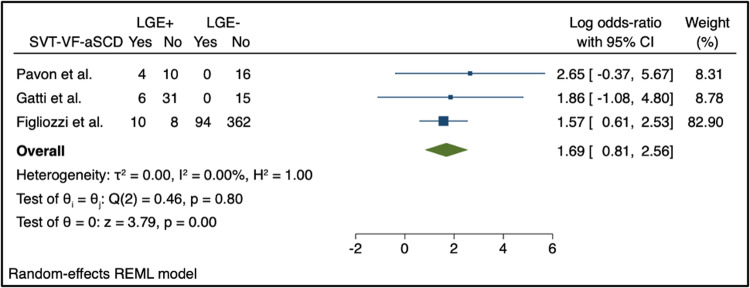
Results: The meta-analysis included 11 studies with 1278 patients. MR severity, leaflet length/thickness, curling, MAD distance, and mapping techniques were not meta-analyzed as reported in < 3 studies. LV end-diastolic volume index, LV ejection fraction, and prolapse distance showed small non-significant effect sizes. LGE showed a strong and significant association with co-VA with a LogORs of 2.12 (95% confidence interval (CI): [1.00, 3.23]), for MAD the log odds-ratio was 0.95 (95% CI: [0.30, 1.60]). The predictive accuracy of LGE was substantial, with a hierarchical summary ROC AUC of 0.83 (95% CI: [0.69, 0.91]) and sensitivity and specificity rates of 0.70 (95% CI: [0.41, 0.89]) and 0.80 (95% CI: [0.67, 0.89]), respectively.
Conclusions: Our study highlights the role of LGE as the key CMR feature for arrhythmia risk stratification in MVP patients. MAD might complement arrhythmic risk stratification.
Clinical relevance statement: LGE is a key factor for arrhythmogenic risk in MVP patients, with additional contribution from MAD. Combining MRI findings with clinical characteristics is critical for evaluating and accurately stratifying arrhythmogenic risk in MVP patients.
Key points: MVP affects 2-3% of the population, with some facing increased risk for arrhythmia. LGE can assess arrhythmia risk, and MAD may further stratify patients. CMR is critical for MVP arrhythmia risk stratification, making it essential in a comprehensive evaluation.
Keywords: Cardiac magnetic resonance imaging; Fibrosis; Mitral valve prolapse; Risk stratification; Ventricular arrhythmias.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

Similar articles
-
Myocardial extracellular volume by T1 mapping: a new marker of arrhythmia in mitral valve prolapse.J Cardiovasc Magn Reson. 2021 Sep 13;23(1):102. doi: 10.1186/s12968-021-00797-2. J Cardiovasc Magn Reson. 2021. PMID: 34517908 Free PMC article.
-
Usefulness of cardiac magnetic resonance images for prediction of sudden cardiac arrest in patients with mitral valve prolapse: a multicenter retrospective cohort study.BMC Cardiovasc Disord. 2021 Nov 17;21(1):546. doi: 10.1186/s12872-021-02362-2. BMC Cardiovasc Disord. 2021. PMID: 34789163 Free PMC article.
-
Imaging for the assessment of the arrhythmogenic potential of mitral valve prolapse.Eur Radiol. 2024 Jul;34(7):4243-4260. doi: 10.1007/s00330-023-10413-9. Epub 2023 Dec 11. Eur Radiol. 2024. PMID: 38078997 Free PMC article. Review.
-
Cardiac magnetic resonance in patients with mitral valve prolapse: Focus on late gadolinium enhancement and T1 mapping.Eur Radiol. 2019 Mar;29(3):1546-1554. doi: 10.1007/s00330-018-5634-5. Epub 2018 Aug 7. Eur Radiol. 2019. PMID: 30088066
-
The Association Between Late Gadolinium Enhancement by Cardiac Magnetic Resonance and Ventricular Arrhythmia in Patients With Mitral Valve Prolapse: A Systematic Review and Meta-Analysis.Clin Cardiol. 2024 Jul;47(7):e24316. doi: 10.1002/clc.24316. Clin Cardiol. 2024. PMID: 38958255 Free PMC article.
Cited by
-
Primary mitral regurgitation, surgery in the transcatheter era: when the neighbourhood becomes noisy: a state-of-art review.Eur Heart J Imaging Methods Pract. 2025 Apr 9;3(1):qyaf041. doi: 10.1093/ehjimp/qyaf041. eCollection 2025 Jan. Eur Heart J Imaging Methods Pract. 2025. PMID: 40342830 Free PMC article. Review.
References
-
- Hayek E, Gring CN, Griffin BP (2005) Mitral valve prolapse. Lancet 365:507–518. 10.1016/S0140-6736(05)17869-6 - PubMed
-
- Freed LA, Levy D, Levine RA et al (1999) Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med 341:1–7. 10.1056/NEJM199907013410101 - PubMed
-
- Nalliah CJ, Mahajan R, Elliott AD et al (2019) Mitral valve prolapse and sudden cardiac death: a systematic review and meta-analysis. Heart 105:144–151. 10.1136/heartjnl-2017-312932 - PubMed
-
- Basso C, Iliceto S, Thiene G, Perazzolo Marra M (2019) Mitral valve prolapse, ventricular arrhythmias, and sudden death. Circulation 140:952–964. 10.1161/CIRCULATIONAHA.118.034075 - PubMed
-
- Sabbag A, Essayagh B, Barrera JDR et al (2022) EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed cby the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. Europace 24:1981–2003. 10.1093/europace/euac125 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
