

Morbidity profile and pharmaceutical management of adult outpatients between primary and tertiary care levels in Sri Lanka: a dual-centre, comparative study
- PMID: 38844839
- PMCID: PMC11155019
- DOI: 10.1186/s12875-024-02448-8
Morbidity profile and pharmaceutical management of adult outpatients between primary and tertiary care levels in Sri Lanka: a dual-centre, comparative study
Abstract
Background: Outpatient care is central to both primary and tertiary levels in a health system. However, evidence is limited on outpatient differences between these levels, especially in South Asia. This study aimed to describe and compare the morbidity profile (presenting morbidities, comorbidities, multimorbidity) and pharmaceutical management (patterns, indicators) of adult outpatients between a primary and tertiary care outpatient department (OPD) in Sri Lanka.
Methods: A comparative study was conducted by recruiting 737 adult outpatients visiting a primary care and a tertiary care facility in the Kandy district. A self-administered questionnaire and a data sheet were used to collect outpatient and prescription data. Following standard categorisations, Chi-square tests and Mann‒Whitney U tests were employed for comparisons.
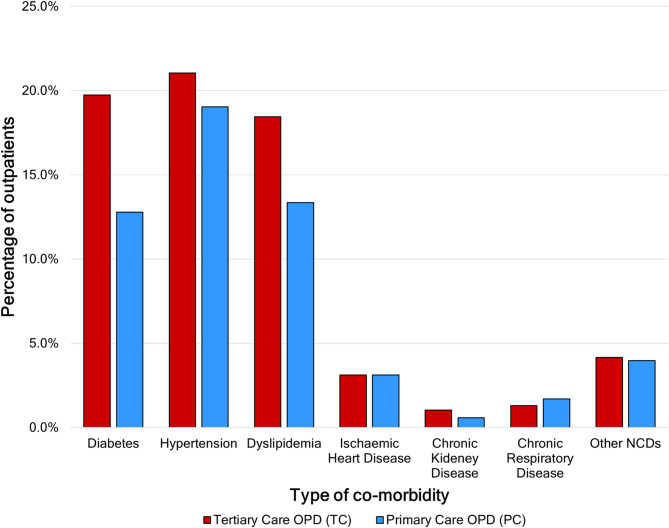
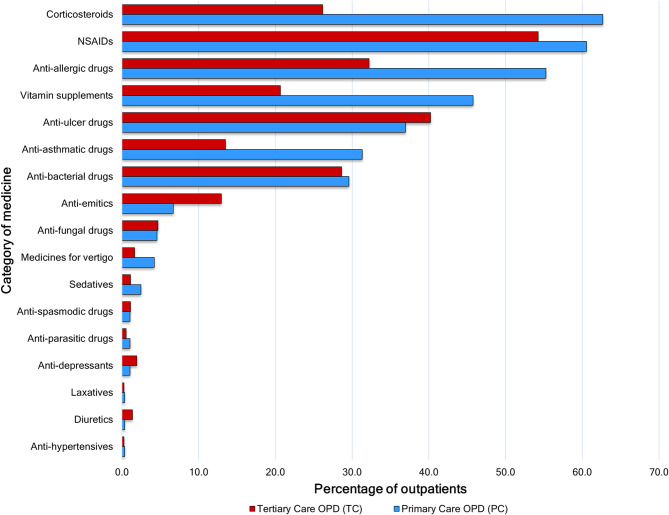
Results: Outpatient cohorts were predominated by females and middle-aged individuals. The median duration of presenting symptoms was higher in tertiary care OPD (10 days, interquartile range: 57) than in primary care (3 days, interquartile range: 12). The most common systemic complaint in primary care OPD was respiratory symptoms (32.4%), whereas it was dermatological symptoms (30.2%) in tertiary care. The self-reported prevalence of noncommunicable diseases (NCDs) was 37.9% (95% CI: 33.2-42.8) in tertiary care OPD and 33.2% (95% CI: 28.5-38.3) in primary care; individual disease differences were significant only for diabetes (19.7% vs. 12.8%). The multimorbidity in tertiary care OPD was 19.0% (95% CI: 15.3-23.1), while it was 15.9% (95% CI: 12.4-20.0) in primary care. Medicines per encounter at primary care OPD (3.86, 95% CI: 3.73-3.99) was higher than that at tertiary care (3.47, 95% CI: 3.31-3.63). Medicines per encounter were highest for constitutional and respiratory symptoms in both settings. Overall prescribing of corticosteroids (62.7%), vitamin supplements (45.8%), anti-allergic (55.3%) and anti-asthmatic (31.3%) drugs was higher in the primary care OPD, and the two former drugs did not match the morbidity profile. The proportion of antibiotics prescribed did not differ significantly between OPDs. Subgroup analyses of drug categories by morbidity largely followed these overall differences.
Conclusions: The morbidities between primary and tertiary care OPDs differed in duration and type but not in terms of multimorbidity or most comorbidities. Pharmaceutical management also varied in terms of medicines per encounter and prescribed categories. This evidence supports planning in healthcare and provides directions for future research in primary care.
Keywords: Disease burden; Health system; Rational prescribing; Reasons for encounter; South Asia; Treatment patterns.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Insights into the morbidity profiles of epidemiologically excluded COVID-19 patients in primary care settings during the third wave of the pandemic in the Anuradhapura District, Sri Lanka.BMC Prim Care. 2025 Apr 3;26(1):95. doi: 10.1186/s12875-025-02792-3. BMC Prim Care. 2025. PMID: 40181290 Free PMC article.
-
Point-prevalence survey of outpatient antibiotic prescription at a tertiary medical center in Sri Lanka: opportunities to improve prescribing practices for respiratory illnesses.BMC Infect Dis. 2021 Jan 21;21(1):97. doi: 10.1186/s12879-021-05804-6. BMC Infect Dis. 2021. PMID: 33478430 Free PMC article.
-
Antibiotic overuse for acute respiratory tract infections in Sri Lanka: a qualitative study of outpatients and their physicians.BMC Fam Pract. 2017 Mar 16;18(1):37. doi: 10.1186/s12875-017-0619-z. BMC Fam Pract. 2017. PMID: 28302056 Free PMC article.
-
Improving the leptospirosis disease burden assessment by including ambulatory patients from outpatient departments: a cross-sectional study.F1000Res. 2020 Sep 14;9:1129. doi: 10.12688/f1000research.26202.2. eCollection 2020. F1000Res. 2020. PMID: 34123371 Free PMC article.
-
Disease Burden Assessment Beyond In-patient Data: A Morbidity Profile Assessment of Outpatients.Int J Prev Med. 2012 Oct;3(10):730-2. Int J Prev Med. 2012. PMID: 23112901 Free PMC article.
Cited by
-
Clinical factors associated with multimorbidity, polypharmacy and medication regimen complexity among adults with hypertension: a multicentre cross-sectional study.BMJ Open. 2025 Apr 10;15(4):e091997. doi: 10.1136/bmjopen-2024-091997. BMJ Open. 2025. PMID: 40216427 Free PMC article.
-
Insights into the morbidity profiles of epidemiologically excluded COVID-19 patients in primary care settings during the third wave of the pandemic in the Anuradhapura District, Sri Lanka.BMC Prim Care. 2025 Apr 3;26(1):95. doi: 10.1186/s12875-025-02792-3. BMC Prim Care. 2025. PMID: 40181290 Free PMC article.
References
-
- Organization WH. Declaration of alma-ata. World Health Organization. Regional Office for Europe; 1978.
-
- Imran SA, Chu K, Rajaraman M, Rajaraman D, Ghosh S, De Brabandere S, et al. Rimary versus Tertiary Care Follow-Up of low-risk differentiated thyroid Cancer: real-world comparison of outcomes and costs for patients and Health Care SystemsP. Eur Thyroid J. 2019;8(4):208–14. doi: 10.1159/000494835. - DOI - PMC - PubMed
-
- Agwanda RO, Kwamanga DO, Kiugu SK. Essential drugs supply and usage as a reflection of outpatient morbidity in Kirinyaga District, Kenya. East Afr Med J. 1996;73(2):120–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources