

Current perspectives in obesity management: unraveling the impact of different therapy approach in real life obesity care
- PMID: 38844956
- PMCID: PMC11155047
- DOI: 10.1186/s12967-024-05322-4
Current perspectives in obesity management: unraveling the impact of different therapy approach in real life obesity care
Abstract
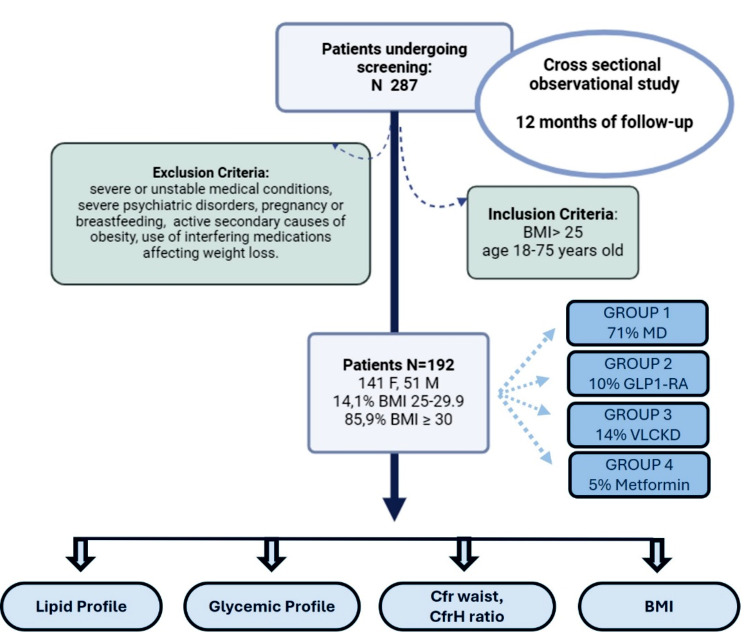
Background: The challenge of addressing obesity persists in healthcare, necessitating nuanced approaches and personalized strategies. This study aims to evaluate the effects of diverse therapeutic interventions on anthropometric and biochemical parameters in individuals with overweight and obesity within a real-world clinical context.
Methods: A retrospective analysis was conducted on 192 patients (141 females, 51 males) aged 18 to 75, with a BMI ranging from 25 to 30 (14.1%) and BMI ≥ 30 (85.9%), observed over a 12-month period at our Endocrinology Unit. Treatment cohorts comprised individuals following different regimens: Mediterranean Diet (MD), with an approximate daily intake of 1500 kcal for women and 1800 kcal for men (71% patients); Ketogenic Diet (KD), utilizing the VLCKD protocol characterized by a highly hypocaloric dietary regimen < 800 kcal/day (14% patients); metformin, administered using the oral formulation (5% patients); pharmacological intervention with GLP1-RA administered via subcutaneous injection with incremental dosage (10% patients). Supply constraints limited the efficacy of Liraglutide, whereas Semaglutide was excluded from comparisons due to its unavailability for obesity without diabetes. Blood tests were conducted to assess lipid profile, glycemic profile, and anthropometric parameters, including BMI, waist circumference, and waist-to-height ratio.
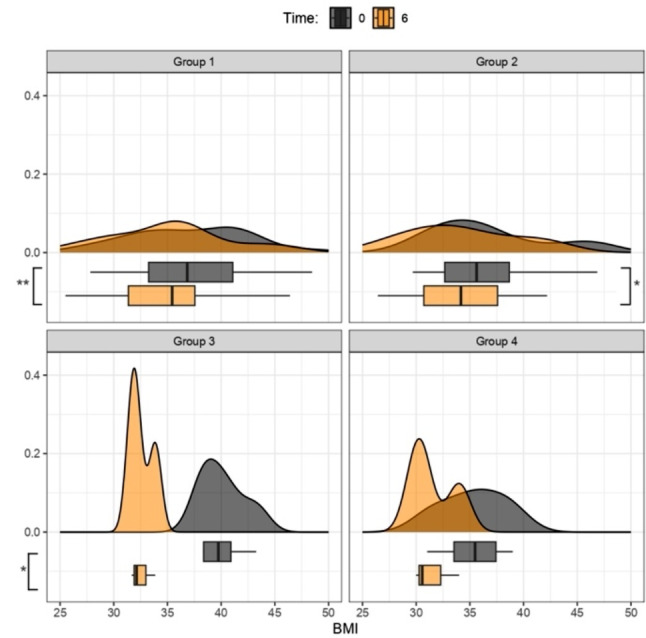
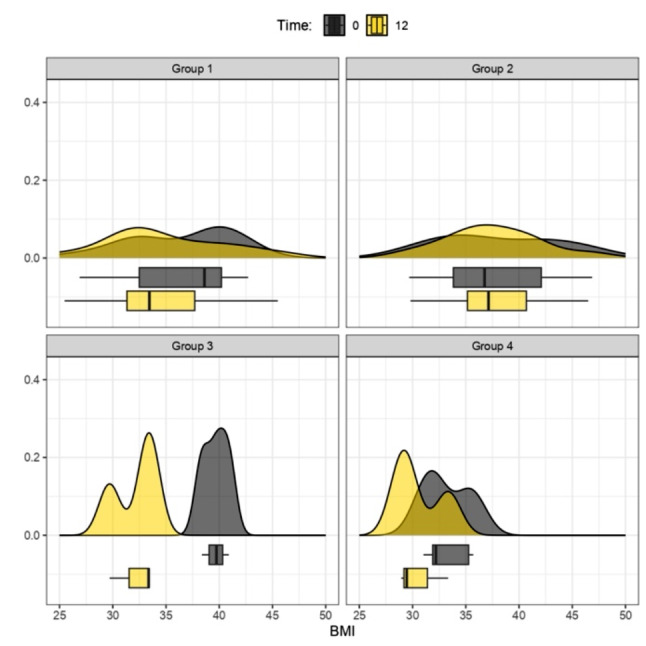
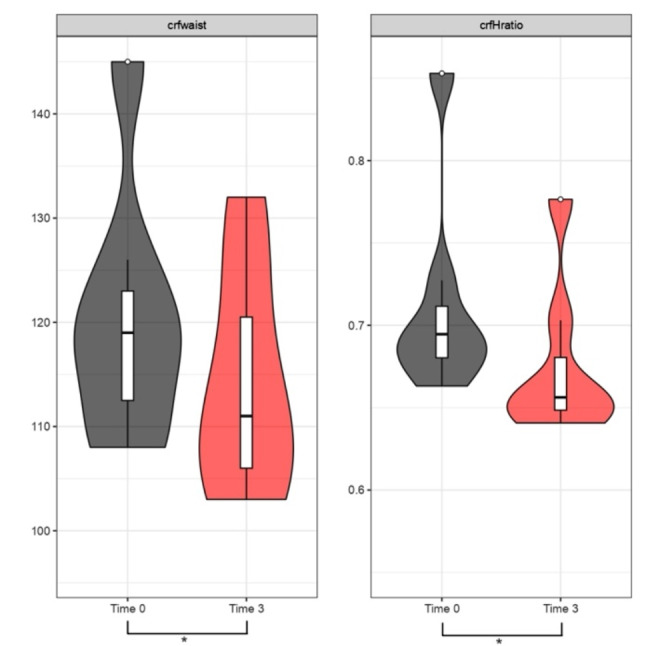
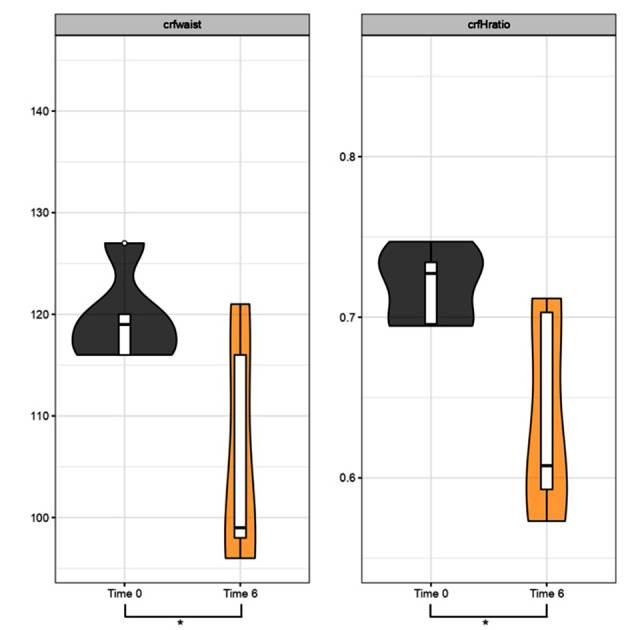
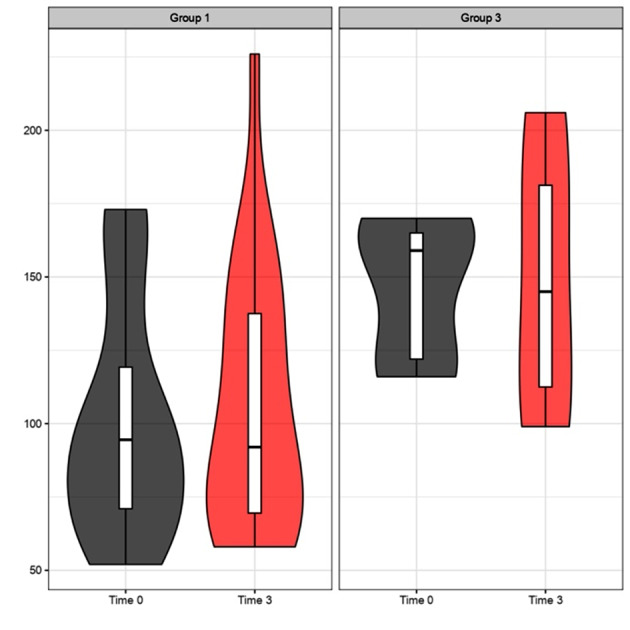
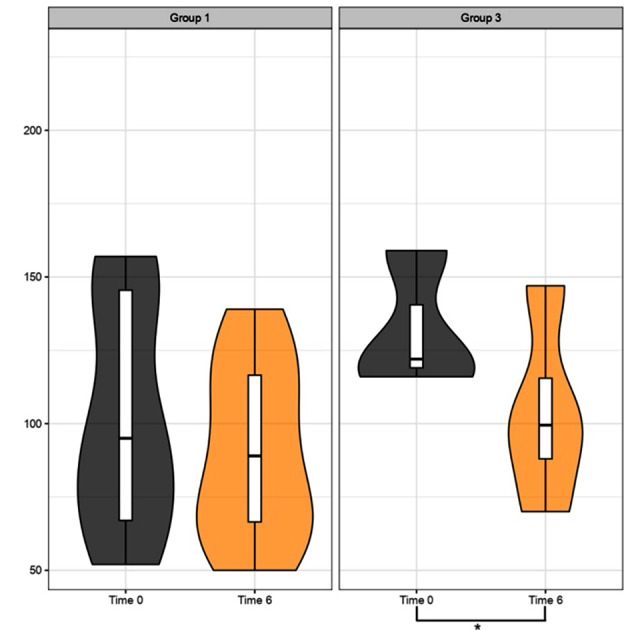
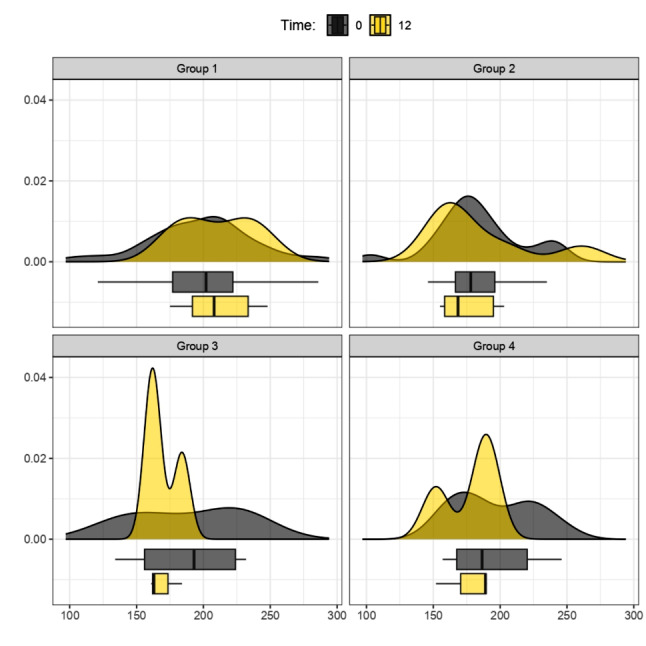
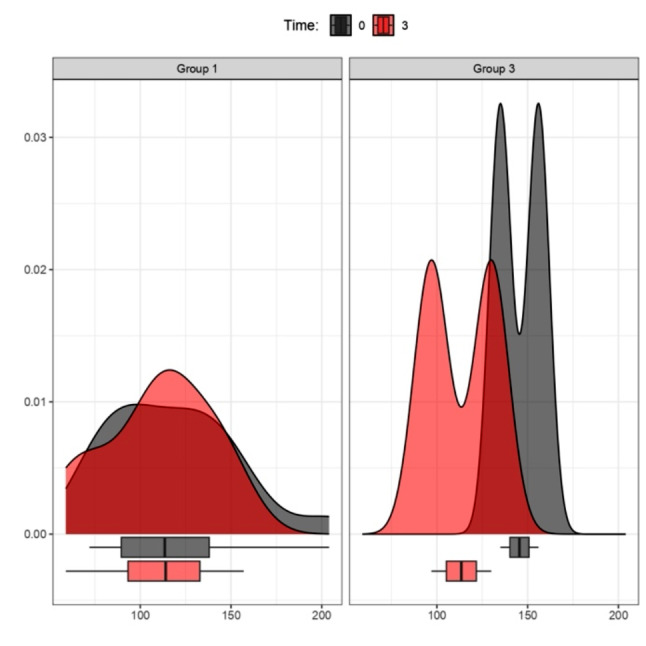
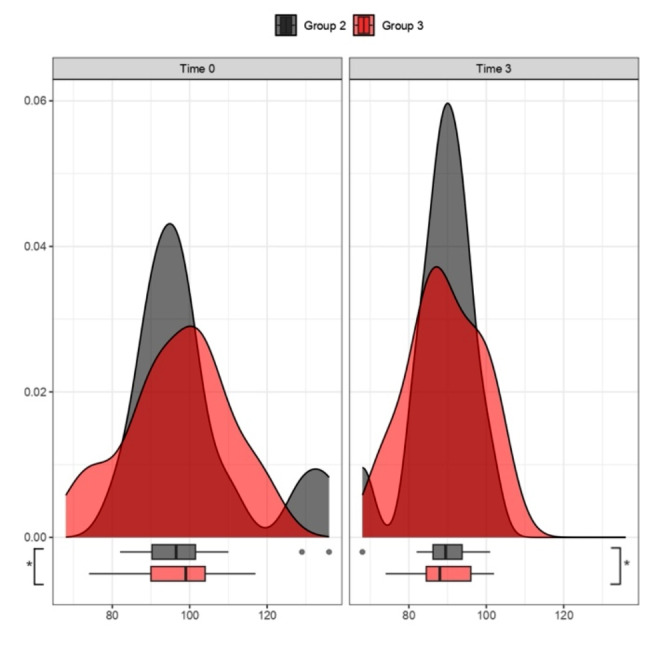
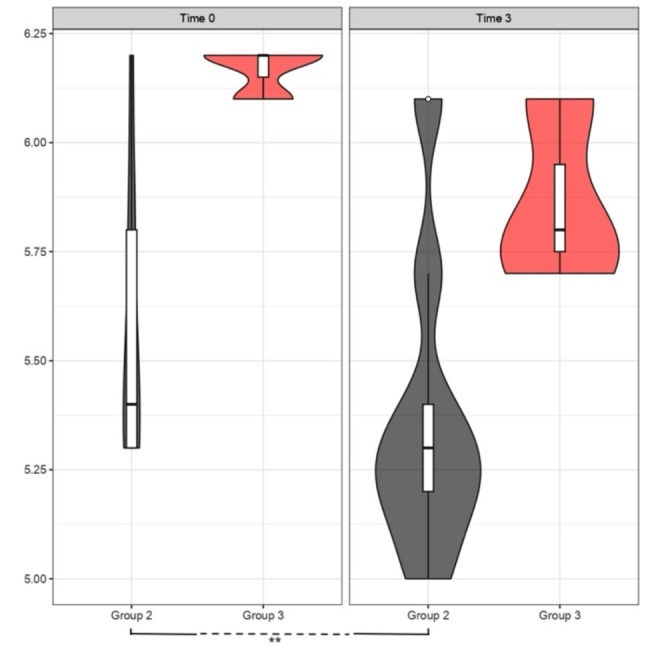
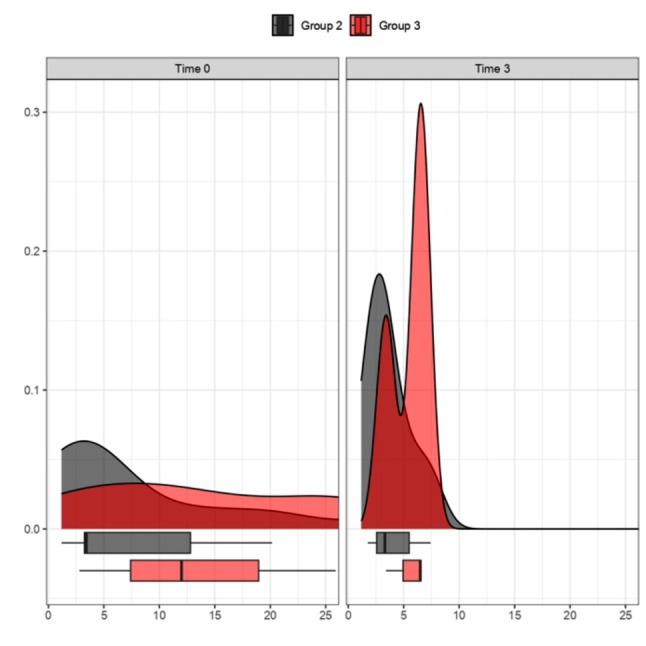
Results: Significant BMI changes were observed from baseline to 6 months across MD, KD, and Liraglutide groups (p < 0.05). KD exhibited notable reductions in waist circumference and waist-to-height ratio within the initial quarter (p < 0.05), with a significant triglyceride decrease after 6 months (p < 0.05), indicating its efficacy over MD. Liraglutide demonstrated a substantial reduction in HbA1c levels in the first quarter (p < 0.05). During the first three months, the ANOVA test on fasting blood glucose showed a statistically significant impact of the time variable (p < 0.05) rather than the specific treatments themselves (Liraglutide and KD), suggesting that adherence during the early stages of therapy may be more critical than treatment choice.
Conclusions: Positive outcomes from targeted interventions, whether pharmacological or dietary should encourage the exploration of innovative, long-term strategies that include personalized treatment alternation. The absence of standardized protocols underscores the importance of careful and tailored planning in managing obesity as a chronic condition.
Keywords: Anti-obesity medications; Glycemic profile; Ketogenic diet; Lipid profile; Metabolic parameters; Weight loss interventions.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bray GA, Kim KK, Wilding JPH, Federation WO. ‘Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation’, Obes Rev, vol. 18, no. 7, pp. 715–723, Jul. 2017, 10.1111/obr.12551. - PubMed
-
- Després J-P, Lemieux I. ‘Abdominal obesity and metabolic syndrome’, Nature, vol. 444, no. 7121, Art. no. 7121, Dec. 2006, 10.1038/nature05488. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
