

Diagnosis and treatment of bacterial peritonitis in patients with gastrointestinal cancer: an observational multicenter study
- PMID: 38845791
- PMCID: PMC11155326
- DOI: 10.1177/17588359241258440
Diagnosis and treatment of bacterial peritonitis in patients with gastrointestinal cancer: an observational multicenter study
Abstract
Background: Bacterial peritonitis (BP) in patients with gastrointestinal (GI) cancer has been poorly described, and its prevalence is unknown.
Objectives: This study aimed to evaluate in patients with both GI cancer and ascites the prevalence of BP, associated features, mechanisms, prognosis, and the diagnostic performance of neutrophil count in ascites.
Design: A retrospective, multicenter, observational study.
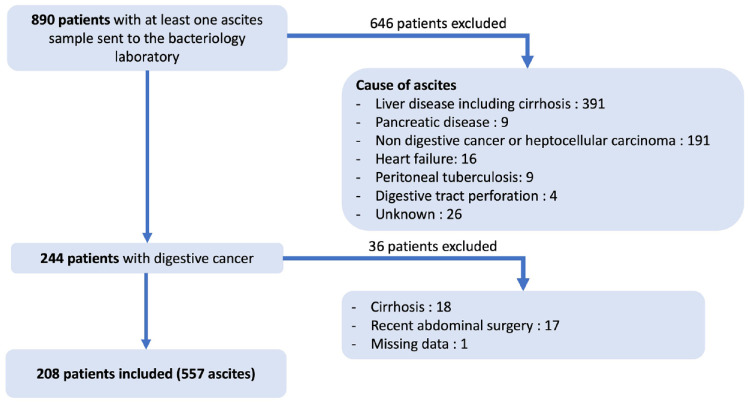
Methods: All patients with GI cancer and ascites who underwent at least one paracentesis sample analyzed for bacteriology over a 1-year period were included. BP was defined by a positive ascites culture combined with clinical and/or biological signs compatible with infection. Secondary BP was defined as BP related to a direct intra-abdominal infectious source.
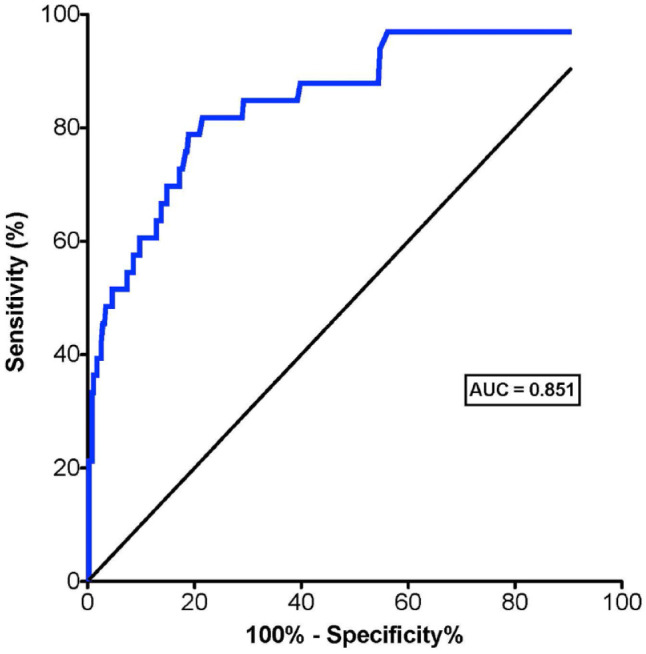
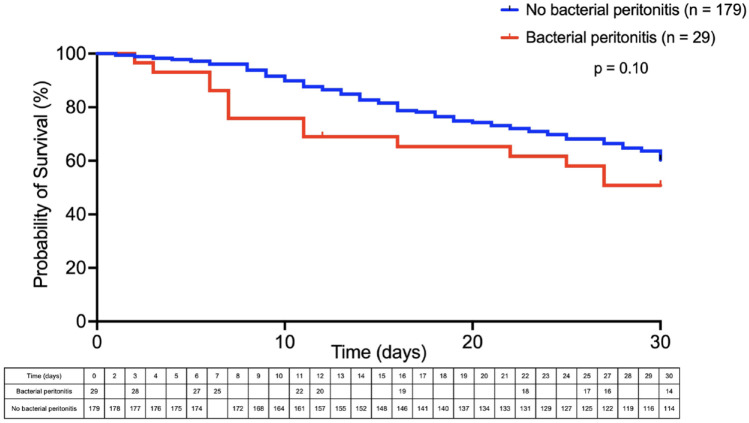
Results: Five hundred fifty-seven ascites from 208 patients included were analyzed. Twenty-eight patients had at least one episode of BP and the annual prevalence rate of BP was 14%. Among the 28 patients with BP, 19 (65%) patients had proven secondary BP and 17 (59%) patients had multi-microbial BP, mainly due to Enterobacterales. A neutrophil count greater than 110/mm3 in ascites had negative and positive predictive values of 96% and 39%, respectively, for the diagnosis of BP. The median survival of patients with BP was 10 days (interquartile range 6-40) after the diagnosis.
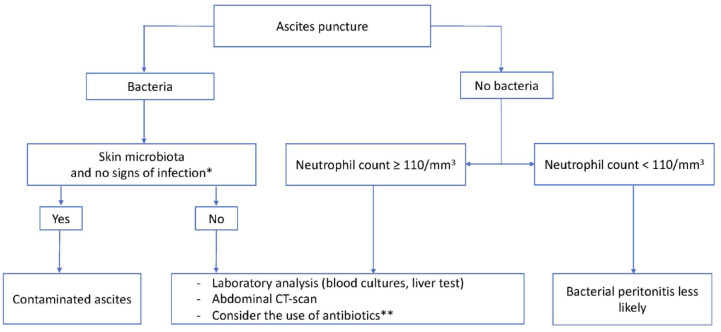
Conclusion: BP is not rare in patients with GI cancer and is associated with a poor short-term prognosis. When a patient with GI cancer is diagnosed with BP, a secondary cause should be sought. Further studies are needed to better define the best management of these patients.
Keywords: Enterobacterales; ascites; diagnosis; infection; malignant ascites; secondary bacterial peritonitis.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Usefulness of routine analysis of ascitic fluid at the time of therapeutic paracentesis in asymptomatic outpatients. Results of a multicenter prospective study.Gastroenterol Clin Biol. 2005 Mar;29(3):275-9. doi: 10.1016/s0399-8320(05)80761-4. Gastroenterol Clin Biol. 2005. PMID: 15864178
-
Spontaneous bacterial peritonitis.Dis Mon. 1985 Sep;31(9):1-48. doi: 10.1016/0011-5029(85)90002-1. Dis Mon. 1985. PMID: 3899555 Review.
-
EUS-guided paracentesis for the diagnosis of malignant ascites.Gastrointest Endosc. 2006 Dec;64(6):908-13. doi: 10.1016/j.gie.2005.11.058. Gastrointest Endosc. 2006. PMID: 17140897
-
[Spontaneous bacterial peritonitis (SBP). Retrospective and prospective data from a multicenter study on prevalence, diagnosis and therapy in Germany].Dtsch Med Wochenschr. 2004 Aug 20;129(34-35):1792-7. doi: 10.1055/s-2004-829030. Dtsch Med Wochenschr. 2004. PMID: 15314741 German.
-
Does this patient have bacterial peritonitis or portal hypertension? How do I perform a paracentesis and analyze the results?JAMA. 2008 Mar 12;299(10):1166-78. doi: 10.1001/jama.299.10.1166. JAMA. 2008. PMID: 18334692 Review.
References
-
- McHutchison JG. Differential diagnosis of ascites. Semin Liver Dis 1997; 17: 191–202. - PubMed
-
- Smith EM, Jayson GC. The current and future management of malignant ascites. Clin Oncol (R Coll Radiol) 2003; 15: 59–72. - PubMed
-
- Ayantunde AA, Parsons SL. Pattern and prognostic factors in patients with malignant ascites: a retrospective study. Ann Oncol 2007; 18: 945–949. - PubMed
-
- Garrison RN, Galloway RH, Heuser LS. Mechanisms of malignant ascites production. J Surg Res 1987; 42: 126–132. - PubMed
-
- Pandya KJ, Whitehead R, Crowley J, et al.. Hyperaldosteronism associated with liver metastases. JAMA 1980; 244: 171–172. - PubMed
LinkOut - more resources
Full Text Sources
