

Surgical treatment algorithm for breast cancer lymphedema-a systematic review
- PMID: 38845835
- PMCID: PMC11150198
- DOI: 10.21037/gs-23-503
Surgical treatment algorithm for breast cancer lymphedema-a systematic review
Abstract
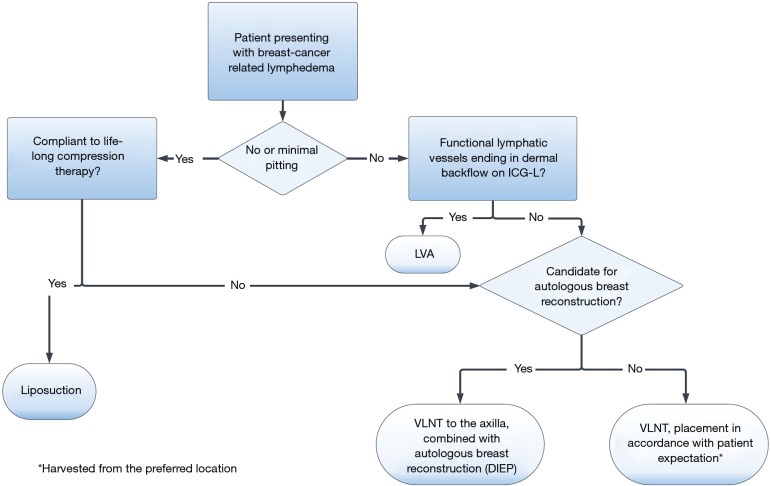
Background: Various surgical treatments are increasingly adopted and gaining popularity for lymphedema treatment. However, challenges persist in selecting appropriate treatment modalities targeted for individual patients and achieving consensus on choice of treatment as well as outcomes. The systematic review aimed to create a treatment algorithm incorporating the latest scientific knowledge, to provide healthcare professionals and patients with a tool for informed decision-making, when selecting between treatments or combining them in a relevant manner. This systematic review evaluated and synthesized the evidence on the effectiveness of three surgical treatments for breast cancer-related lymphedema (BCRL): lymphovenous anastomosis (LVA), vascularized lymph node transfer (VLNT), and liposuction.
Methods: We conducted a systematic search of electronic databases on 18 June 2023, including Medline, Embase, Cochrane Library, Google Scholar, and ClinicalTrials.org. Eligible studies were randomized controlled trials, non-randomized comparative studies, and observational studies that assessed the outcomes of LVA, VLNT, or liposuction in managing BCRL. The primary results of interest were changes in arm volume, lymphatic flow, and quality of life. Two independent reviewers performed the study selection and data extraction. Following this, we systematically reviewed and conducted a risk of bias assessment. Results were qualitatively presented, and a treatment algorithm was developed based on the available data.
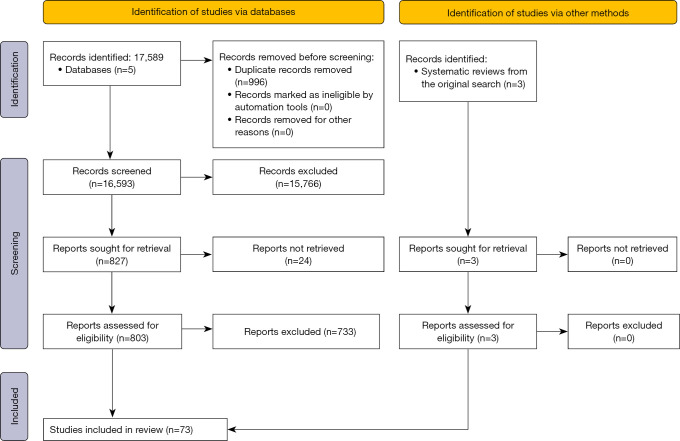
Results: We identified 16,593 papers, after removal of duplicates. Following assessment of studies, 73 articles met the inclusion criteria, including 2,373 patients. We were not able to conduct a meta-analysis due to considerable heterogeneity in the methodologies and outcome measures across the studies. Liposuction appears effective for patients presenting with non-pitting lymphedema. LVA indicates variable success rate, with some evidence indicating a reduction in limb volume and symptomatic relief amongst early stages of lymphedema. VLNT showed promising results for limb volume reduction and symptom improvement in patients presenting with mild and moderate lymphedema.
Conclusions: Liposuction, LVA, and VLNT seem to be effective treatments for BCRL, when targeted for the appropriate patient. Well-conducted high evidence clinical studies in the field are still lacking to uncover the efficacy of surgical treatment for BCRL.
Keywords: Breast cancer-related lymphedema (BCRL); liposuction; lymphovenous anastomosis (LVA); secondary lymphedema; vascularized lymph node transfer (VLNT).
2024 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://gs.amegroups.org/article/view/10.21037/gs-23-503/coif). The series “Hot Topics in Breast Reconstruction World Wide” was commissioned by the editorial office without any funding or sponsorship. Funding originated from the ACROBATIC—Research Collaboration Across Surgical Oncology for Better Patient Care, Danish Cancer Society (No. R317-A18255) and Danish Comprehensive Cancer Center Report covers 1 year salary for the first author (C.L.) during her PhD. study. T.E.D. served as the unpaid guest editor of the series and is a committee member of ACROBATIC—Research Collaboration Across Surgical Oncology for Better Patient Care, who has financially supported the main author of this article. J.B.T. serves as an unpaid Honorary Editor-in-Chief of Gland Surgery from November 2022 to October 2024 and served as the unpaid guest editor of the series. The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Outcomes of Lymphovenous Anastomoses and Vascularized Lymph Node Transplant in the Combined Surgical Treatment of Lymphedema: A Prospective Cohort Study.Plast Reconstr Surg. 2025 Jul 22. doi: 10.1097/PRS.0000000000012326. Online ahead of print. Plast Reconstr Surg. 2025. PMID: 40707214
-
Improving quality of life after breast cancer: a comparison of two microsurgical treatment options for breast cancer-related lymphedema (BCRL).Clin Exp Med. 2024 Apr 23;24(1):82. doi: 10.1007/s10238-024-01344-w. Clin Exp Med. 2024. PMID: 38653874 Free PMC article.
-
Vascularized lymph node transfer (VLNT) versus lymphaticovenous anastomosis (LVA) for chronic breast cancer-related lymphedema (BCRL): a retrospective cohort study of effectiveness over time.Breast Cancer Res Treat. 2025 Apr;210(2):319-327. doi: 10.1007/s10549-024-07567-5. Epub 2024 Dec 10. Breast Cancer Res Treat. 2025. PMID: 39653884 Free PMC article.
-
Microsurgical techniques in the treatment of breast cancer-related lymphedema: a systematic review of efficacy and patient outcomes.Breast Cancer. 2021 Sep;28(5):1002-1015. doi: 10.1007/s12282-021-01274-5. Epub 2021 Jul 12. Breast Cancer. 2021. PMID: 34254232 Free PMC article.
-
Surgical treatment of breast cancer related lymphedema-the combined approach: a literature review.Gland Surg. 2023 Dec 26;12(12):1746-1759. doi: 10.21037/gs-23-247. Epub 2023 Dec 22. Gland Surg. 2023. PMID: 38229846 Free PMC article. Review.
Cited by
-
[An overview of integrated surgical management for secondary lower limb lymphedema guided by algorithms].Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025 Jun 20;41(6):516-524. doi: 10.3760/cma.j.cn501225-20250217-00067. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025. PMID: 40480841 Free PMC article. Chinese.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous