

[Results of emergency management of esophageal lesions related to caustic ingestion in children in the emergency department of the General Reference Hospital of Niamey (Niger)]
- PMID: 38846116
- PMCID: PMC11151903
- DOI: 10.48327/mtsi.v4i1.2024.399
[Results of emergency management of esophageal lesions related to caustic ingestion in children in the emergency department of the General Reference Hospital of Niamey (Niger)]
Abstract
Introduction: Caustic ingestion in children is a public health problem; it is mainly due to domestic accidents due to improper packaging and storage of caustic products. It is a medical and surgical emergency whose management is multidisciplinary. The lesions caused by the accidental ingestion of caustics can affect the functional and vital prognosis in 10% of cases.
Methodology: A retrospective, descriptive study from January 2020 to December 2022 (2 years), carried out in the emergency department of the General Reference Hospital of Niamey (Niger). The study included patients less than 15 years old admitted for ingesting a caustic product.
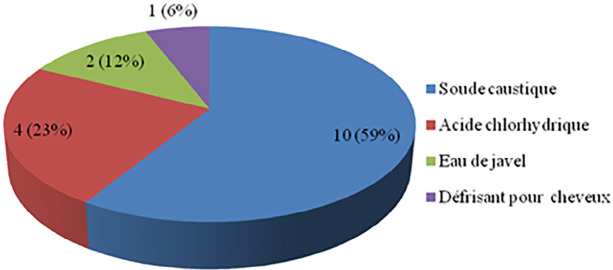
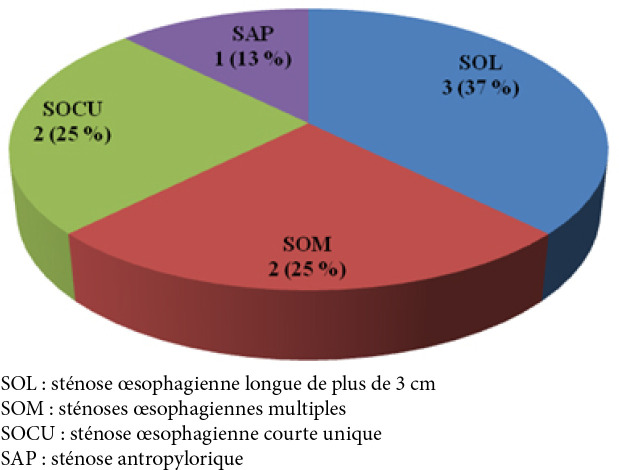
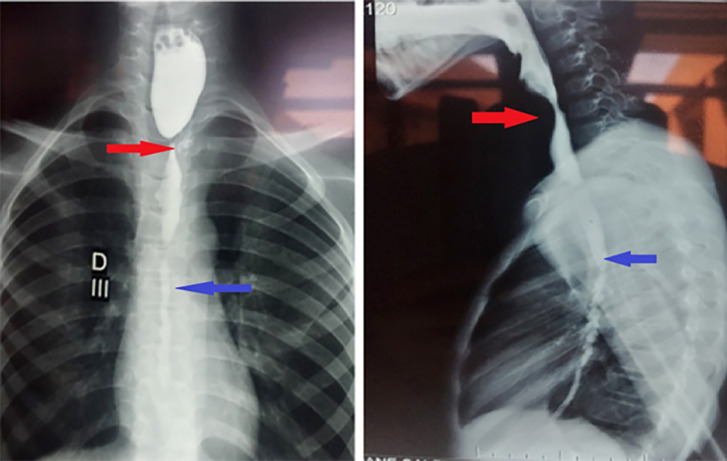
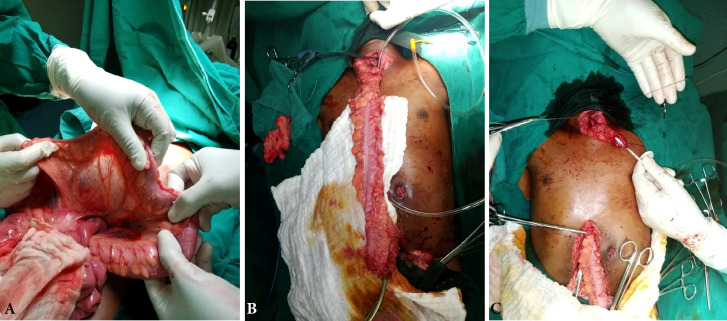
Results: Our study included 17 patients. The average age was 5 years, with age extremes of 2 to 11 years. We noted a male predominance with a sex ratio (M/F) of 2.4. Ingestion of caustic products was accidental in all cases. The caustic product was caustic soda in 59%. The average quantity of product ingested was 5 ml (2 ml to 20 ml). The average consultation time was 3 days (3 hours to 15 days). Clinically, dysphagia was the most functional sign, represented by 13 cases, or 76%. Regarding general signs, 3 patients (18%) were admitted with fever; blood pressure was normal in 15 patients (88%); and 2 patients (18%) were admitted in a state of shock. The respiratory rate was normal in 14 patients (82%). Four patients (24%) were admitted in a state of deterioration in the general condition associated with severe malnutrition and dehydration. On physical examination, 2 patients (12%) presented with abdominal defense at the epigastric level. Examination of the ENT sphere revealed benign buccopharyngeal ulcerations in 2 patients (12%). Esogastroduodenal fibroscopy was performed in 4 patients (24%). The caustic lesions observed in the esophagus were: Zargar stage I at 25%, stage Ila at 50%, and stage Illb at 25%. In the stomach, the lesions were Zargar stage I in 75% of cases and stage III in 25% of cases. An injected thoracic-abdominopelvic computed tomography (CT) was performed in 3 patients (18%). It revealed a lack of enhancement of the esophageal wall compatible with esophageal necrosis in one patient. An esophagogastroduodenal transit was performed in 8 patients (47%) admitted more than 72 hours after ingestion of the caustic. They showed esophageal stenoses longer than 3 cm in 3 patients, multiple esophageal stenoses in 2 patients, a single esophageal stenosis in 2 patients, and a single antropyloric stenosis in 1 patient. Therapeutically, all patients benefited from antiemetics to avoid vomiting and proton pump inhibitors. Intravenous antibiotic prophylaxis with third-generation cephalosporin was administered to 12 patients (71%). Corticosteroid therapy based on IV prednisolone at a dose of 1 g/1.73 m2 per day was used to limit or prevent stenoses in 9 patients (53%). Parenteral nutrition was administered to 7 patients (41%). Endoscopic dilations were performed in 2 patients (12%). Emergency surgical treatment was performed in 7 patients (41%): 3 patients underwent transitional feeding gastrostomies; in 3 others, esophagoplasties by colon transplant were performed, and 1 patient was treated by stripping of the esophagus associated with total gastrectomy. The postoperative course was marked by a leak of esocolic anastomosis in one patient for whom conservative treatment was performed with good progress. The average length of hospital stay was 5 days (1-32 days).
Conclusion: Accidental caustic ingestions can have serious consequences. Preventing these accidents relies on raising public awareness of the dangers associated with improper storage of these products.
Introduction: L'ingestion de produits caustiques chez l'enfant constitue un problème de santé publique; il s'agit essentiellement d'accidents domestiques dus aux mauvais conditionnements et aux stockages de ces produits. C'est une urgence médico-chirurgicale dont la prise en charge est multidisciplinaire. Les lésions occasionnées peuvent engager le pronostic fonctionnel œsophagien et vital dans 10 % des cas.
Méthodologie: Il s'agissait d'une étude rétrospective et analytique, sur une période de 2 ans (janvier 2020 à décembre 2022), réalisée dans le service des urgences de l'Hôpital général de référence de Niamey (Niger). Cette étude avait inclus les patients de moins de 15 ans admis pour ingestion de produit caustique.
Résultats: Notre étude avait inclus 17 patients; l’âge moyen était de 5 ans (2-11 ans); le sexratio (H/F) était de 2,4. La soude caustique était en cause dans 59 % des cas, et le délai moyen de consultation était de 3 jours. La dysphagie était présente dans 76 % des cas. L’état de choc et la dénutrition sévère étaient retrouvés dans respectivement 18 et 24 % des cas. À l'examen abdominal, 12 % des patients présentaient une défense abdominale. L'endoscopie était réalisée chez 4 patients et les lésions sévères œsophagiennes (IIIb de Zargar) étaient retrouvées dans 25 % des cas. Sur le plan thérapeutique, l'antibioprophylaxie et la corticothérapie avaient été réalisées dans respectivement 71 % et 53 % des cas. Les dilatations endoscopiques avaient été réalisées dans 12 % des cas et la chirurgie était indiquée chez 7 patients (41 %) dont 3 gastrostomies d'alimentation transitoires, 3 œsophagoplasties par transplant colique et 1 stripping de l’œsophage.
Conclusion: Les ingestions accidentelles caustiques peuvent avoir des conséquences graves. La prévention de ces accidents repose sur la sensibilisation du public sur les dangers associés au stockage inapproprié de ces produits.
Keywords: Caustic ingestion; Endoscopy; Esophagitis; Esophagoplasty; Hospital; Niamey; Niger; Oesophageal stricture; Sub-Saharan Africa.
Copyright © 2024 SFMTSI.
Conflict of interest statement
Les auteurs ne déclarent aucun lien d'intérêt.
Figures


Similar articles
-
[High doses of steroids in the management of caustic esophageal burns in children].Arch Pediatr. 2004 Jan;11(1):13-7. doi: 10.1016/j.arcped.2003.10.011. Arch Pediatr. 2004. PMID: 14700754 Clinical Trial. French.
-
The results of caustic ingestions.Hepatogastroenterology. 2004 Sep-Oct;51(59):1397-400. Hepatogastroenterology. 2004. PMID: 15362762
-
[Management of caustic esophagitis in children].Arch Pediatr. 2012 Dec;19(12):1362-8. doi: 10.1016/j.arcped.2012.09.013. Epub 2012 Nov 7. Arch Pediatr. 2012. PMID: 23141564 Review. French.
-
Consequences of caustic ingestions in children.Acta Paediatr. 1994 Nov;83(11):1200-5. doi: 10.1111/j.1651-2227.1994.tb18281.x. Acta Paediatr. 1994. PMID: 7841737 Review.
-
[Clinical-epidemiological characteristics in caustics ingestion patients in the Hipólito Unanue National Hospital].Rev Gastroenterol Peru. 2003 Apr-Jun;23(2):115-25. Rev Gastroenterol Peru. 2003. PMID: 12853988 Review. Spanish.
References
-
- Betalli P, Falchetti D, Giuliani S, Pane A, Dall'Oglio L, de Angelis GL, Caldore M, Romano C, Gamba P, Baldo V, Caustic Ingestion Italian Study Group Caustic ingestion in children: Is endoscopy always indicated? The results of an Italian multicenter observational study. Gastrointest Endosc. 2008 Sep;68(3):434–439. doi: 10.1016/j.gie.2008.02.016. - DOI - PubMed
-
- Chirica M, Fieux F, Villa A, Munoz-Bongrand N, Sarfati E, Cattan P. Prise en charge médicochirurgicale des ingestions de caustique du tube digestif haut. EMC (Elsevier Masson, SAS, Paris), Gastro-entérologie. 2011:9-200-A-10.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous