

Case Reports
doi: 10.7759/cureus.59783.
eCollection 2024 May.
The Clinical and Histological Intersection of Cardiac Sarcoidosis and Giant Cell Myocarditis
Affiliations
- PMID: 38846240
- PMCID: PMC11154654
- DOI: 10.7759/cureus.59783
Item in Clipboard
Case Reports
The Clinical and Histological Intersection of Cardiac Sarcoidosis and Giant Cell Myocarditis
Cureus.
.
Abstract
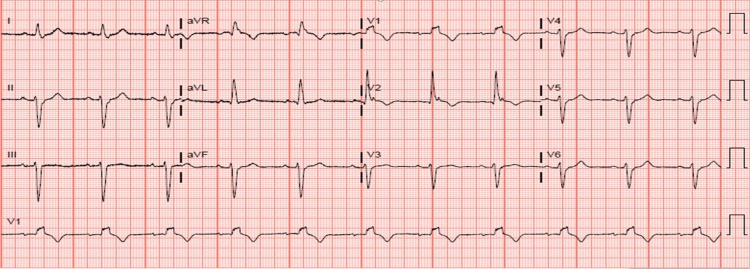
The clinical and imaging features of cardiac sarcoidosis (CS) and giant cell myocarditis (GCM) are occasionally indistinguishable. This is a case of heart block and ventricular tachycardia where cardiac MRI, fluorodeoxyglucose positron emission tomography (FDG-PET) and biopsy revealed intermediate clinicohistologic phenotype between CS and GCM. This highlights gaps in the management of overlap conditions.
Keywords: biopsy; cardiac sarcoidosis; giant cell myocarditis; histology; management; overlap; pet scans.
Copyright © 2024, Sharma et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

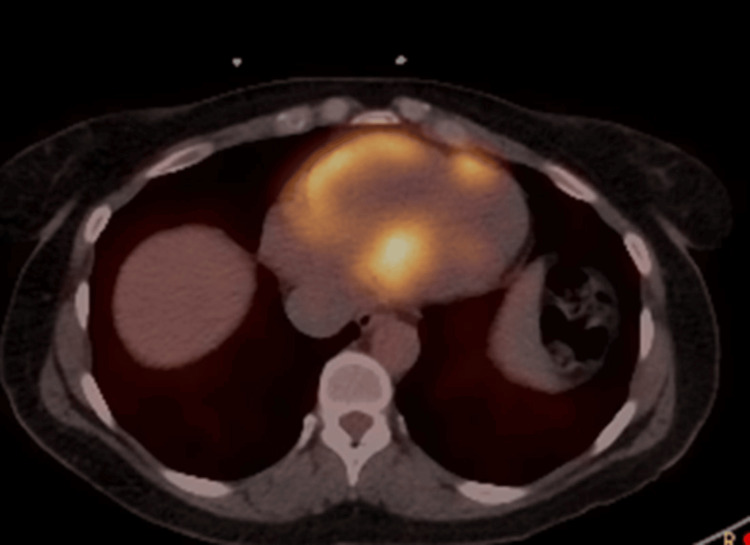
PET: positron emission tomography.
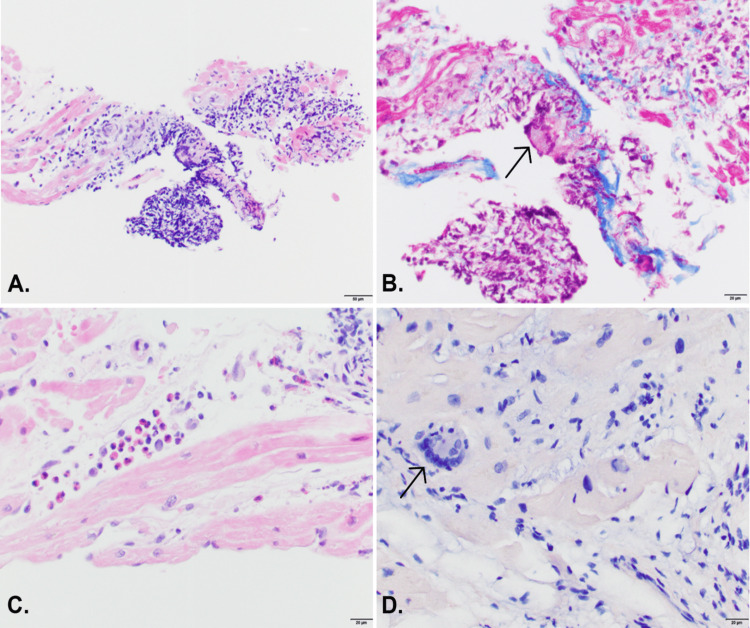
(A) Medium power view (20x) of H&E-stained section shows a focus of mixed inflammatory cells in the myocardium. (B) Trichrome stain (40x) highlights the early fibrosis associated with the focus of inflammation with a rare giant cell (arrow). (C) High power (40x) of H&E-stained section shows a focus of predominantly eosinophils. (D) Congo red-stained section (40x) is negative for amyloid but shows a giant cell (arrow) without granuloma formation. H&E: hematoxylin and eosin.
Similar articles
-
Fulminant cardiac sarcoidosis resembling giant cell myocarditis: a case report.Eur Heart J Case Rep. 2021 Mar 10;5(3):ytab042. doi: 10.1093/ehjcr/ytab042. eCollection 2021 Mar. Eur Heart J Case Rep. 2021. PMID: 33733047 Free PMC article.
-
Giant Cell Myocarditis vs Cardiac Sarcoidosis: Reconsidering the Diagnosis With FDG PET Imaging.JACC Case Rep. 2024 Nov 20;29(22):102738. doi: 10.1016/j.jaccas.2024.102738. eCollection 2024 Nov 20. JACC Case Rep. 2024. PMID: 39691891 Free PMC article.
-
Cardiac sarcoidosis and giant cell myocarditis as causes of atrioventricular block in young and middle-aged adults.Circ Arrhythm Electrophysiol. 2011 Jun;4(3):303-9. doi: 10.1161/CIRCEP.110.959254. Epub 2011 Mar 22. Circ Arrhythm Electrophysiol. 2011. PMID: 21427276
-
Idiopathic giant cell myocarditis and cardiac sarcoidosis.Heart Fail Rev. 2013 Nov;18(6):733-46. doi: 10.1007/s10741-012-9358-3. Heart Fail Rev. 2013. PMID: 23111533 Review.
-
[Inflammatory heart diseases--cardiac sarcoidosis and giant cell myocarditis].Duodecim. 2015;131(22):2127-33. Duodecim. 2015. PMID: 26749906 Review. Finnish.
References
-
- Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. Felker GM, Thompson RE, Hare JM, et al. N Engl J Med. 2000;342:1077–1084. - PubMed
-
- A clinical and histopathologic comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis. Okura Y, Dec GW, Hare JM, et al. J Am Coll Cardiol. 2003;15:322–329. - PubMed
-
- Heart Failure Association, Heart Failure Society of America, and Japanese Heart Failure Society Position Statement on Endomyocardial Biopsy. Seferović PM, Tsutsui H, Mcnamara DM, et al. J Card Fail. 2021;27:727–743. - PubMed
Publication types
LinkOut - more resources
Full Text Sources