

Coronary microvascular dysfunction and myocardial area at risk assessed by cadmium zinc telluride single photon emission computed tomography after primary percutaneous coronary intervention in acute myocardial infarction patients
- PMID: 38846287
- PMCID: PMC11151247
- DOI: 10.21037/qims-23-1260
Coronary microvascular dysfunction and myocardial area at risk assessed by cadmium zinc telluride single photon emission computed tomography after primary percutaneous coronary intervention in acute myocardial infarction patients
Abstract
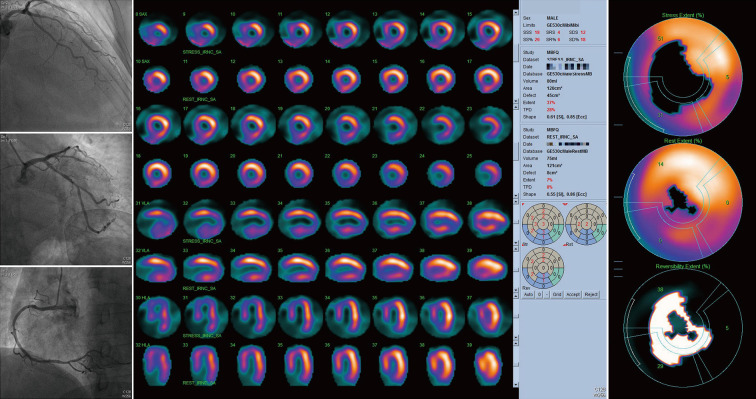
Background: A high proportion of coronary microvascular dysfunction (CMD) has been observed in patients with acute myocardial infarction (AMI) who have received primary percutaneous coronary intervention (PCI), which may affect their prognosis. This study used cadmium zinc telluride (CZT) single photon emission computed tomography (SPECT) to evaluate the prevalence and characteristics of CMD and myocardial area at risk (AAR) in AMI patients who had undergone primary PCI.
Methods: We conducted a single-center cross-sectional retrospective study at TEDA International Cardiovascular Hospital from September 2021 to June 2022. A total of 83 patients received primary PCI for AMI. Subsequently, a rest/stress dynamic and routine gated myocardial perfusion imaging (MPI) were performed 1 week after PCI. The CMD group was defined as having a residual stenosis of infarct-related artery (IRA) <50% and myocardial flow reserve (MFR) <2.0 in this corresponding territory, whereas MFR ≥2.0 of IRA pertained to the normal control group. Rest-AAR of infarction (%) and stress-AAR (%) were expressed by the percentage of measured rest-defect-size and stress-defect-size in the left ventricular area, respectively. Logistic regression analyses were performed to identify significant predictors of CMD.
Results: A total of 53 patients with a mean age of 57.06±11.99 years were recruited, of whom 81.1% were ST-segment elevation myocardial infarction (STEMI). The proportion of patients with CMD was 79.2% (42/53). The time of pain to SPECT imaging was 7.50±1.27 days in the CMD group and 7.45±1.86 days among controls. CMD patients had a higher body mass index (BMI) than controls (26.48±3.26 vs. 24.36±2.73 kg/m2, P=0.053), and a higher proportion of STEMI, thrombolysis in myocardial infarction (TIMI) 0 grade of IRA prior PCI than controls (88.1% vs. 54.5%, P=0.011; 61.9% vs. 18.2%, P=0.004, respectively). No significant difference was identified in the rest-myocardial blood flow (MBF) of IRA between the 2 groups, whereas the stress-MBF and MFR of IRA, rest-AAR, and stress-AAR in the CMD group were remarkably lowered. Higher BMI [odds ratio (OR): 1.332, 95% confidence interval (CI): 1.008-1.760, P=0.044] and stress-AAR (OR: 1.994, 95% CI: 1.122-3.543, P=0.019) were used as independent predictors of CMD occurrence.
Conclusions: The prevalence of CMD is high in AMI patients who received primary PCI. Each 1 kg/m2 increase in BMI was associated with a 1.3-fold increase in CMD risk. A 5% increase in stress-AAR was associated with a nearly 2-fold increase in CMD risk. Increased BMI and stress-AAR predicts decreased coronary reserve function.
Keywords: Coronary microvascular dysfunction (CMD); acute myocardial infarction (AMI); myocardial flow reserve (MFR); percutaneous coronary intervention (PCI); single photon emission computed tomography (SPECT).
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1260/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Prevalence and characteristics of coronary microvascular dysfunction in post-percutaneous coronary intervention patients with recurrent chest pain.Cardiovasc Diagn Ther. 2022 Apr;12(2):166-176. doi: 10.21037/cdt-21-705. Cardiovasc Diagn Ther. 2022. PMID: 35433345 Free PMC article.
-
Significant Association of Serum Albumin With the Severity of Coronary Microvascular Dysfunction Using Dynamic CZT-SPECT.Microcirculation. 2024 Jul;31(5):e12853. doi: 10.1111/micc.12853. Epub 2024 May 1. Microcirculation. 2024. PMID: 38690605
-
[Diagnostic efficiency and incremental value of myocardial blood flow quantification by CZT SPECT for patients with coronary artery disease].Zhonghua Xin Xue Guan Bing Za Zhi. 2022 May 24;50(5):494-500. doi: 10.3760/cma.j.cn112148-20211124-01018. Zhonghua Xin Xue Guan Bing Za Zhi. 2022. PMID: 35589599 Chinese.
-
Myocardial blood flow evaluation with dynamic cadmium-zinc-telluride single-photon emission computed tomography: Bright and dark sides.Diagn Interv Imaging. 2023 Jul-Aug;104(7-8):323-329. doi: 10.1016/j.diii.2023.02.001. Epub 2023 Feb 14. Diagn Interv Imaging. 2023. PMID: 36797156 Review.
-
Advances in the diagnosis and management of post-percutaneous coronary intervention coronary microvascular dysfunction: Insights into pathophysiology and metabolic risk interactions.World J Cardiol. 2025 Feb 26;17(2):103950. doi: 10.4330/wjc.v17.i2.103950. World J Cardiol. 2025. PMID: 40061275 Free PMC article. Review.
Cited by
-
Coronary microvascular dysfunction in post-PCI target vessels: a systematic review and meta-analysis of prevalence and associated outcomes.Front Cardiovasc Med. 2025 Aug 4;12:1620204. doi: 10.3389/fcvm.2025.1620204. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40832144 Free PMC article.
-
Predicting cardiac resynchronization therapy response: development and validation of a single photon emission computed tomography-based nomogram.Quant Imaging Med Surg. 2025 May 1;15(5):4247-4261. doi: 10.21037/qims-2024-2700. Epub 2025 Apr 28. Quant Imaging Med Surg. 2025. PMID: 40384719 Free PMC article.
References
-
- Konijnenberg LSF, Damman P, Duncker DJ, Kloner RA, Nijveldt R, van Geuns RM, Berry C, Riksen NP, Escaned J, van Royen N. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc Res 2020;116:787-805. 10.1093/cvr/cvz301 - DOI - PMC - PubMed
-
- Scarsini R, Shanmuganathan M, De Maria GL, Borlotti A, Kotronias RA, Burrage MK, Terentes-Printzios D, Langrish J, Lucking A, Fahrni G, Cuculi F, Ribichini F, Choudhury RP, Kharbanda R, Ferreira VM, Channon KM, Banning AP; OxAMI Study Investigators. Coronary Microvascular Dysfunction Assessed by Pressure Wire and CMR After STEMI Predicts Long-Term Outcomes. JACC Cardiovasc Imaging 2021;14:1948-59. 10.1016/j.jcmg.2021.02.023 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous