

Role of clinical and multidetector computed tomography (MDCT) features in the prediction of patients with intestinal lipoma developing intussusception
- PMID: 38846289
- PMCID: PMC11151265
- DOI: 10.21037/qims-23-1530
Role of clinical and multidetector computed tomography (MDCT) features in the prediction of patients with intestinal lipoma developing intussusception
Abstract
Background: Intestinal lipoma is considered the most common benign tumor that causes intussusception. This retrospective case-control study aimed to present the clinical and multidetector computed tomography (MDCT) features between intestinal lipomas with and without intussusception and examine risk factors that predict intussusception caused by intestinal lipomas.
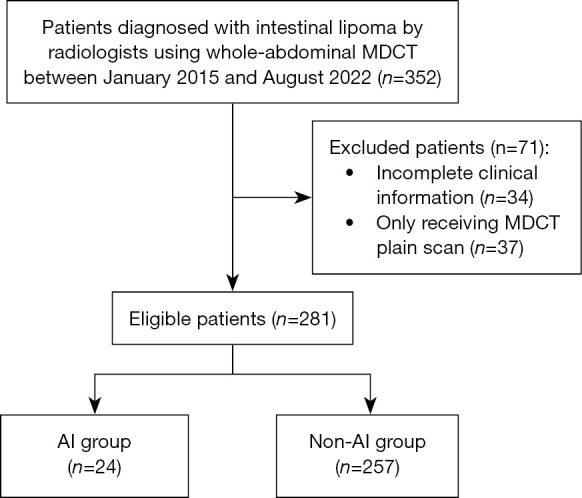
Methods: We retrospectively analyzed 281 adult patients diagnosed with intestinal lipoma by radiologists using whole-abdominal MDCT between January 2015 and August 2022. Patients were divided into adult intussusception (AI) and non-AI groups based on MDCT images. Univariate logistic regression was performed to identify risk factors for intestinal lipoma-induced intussusception.
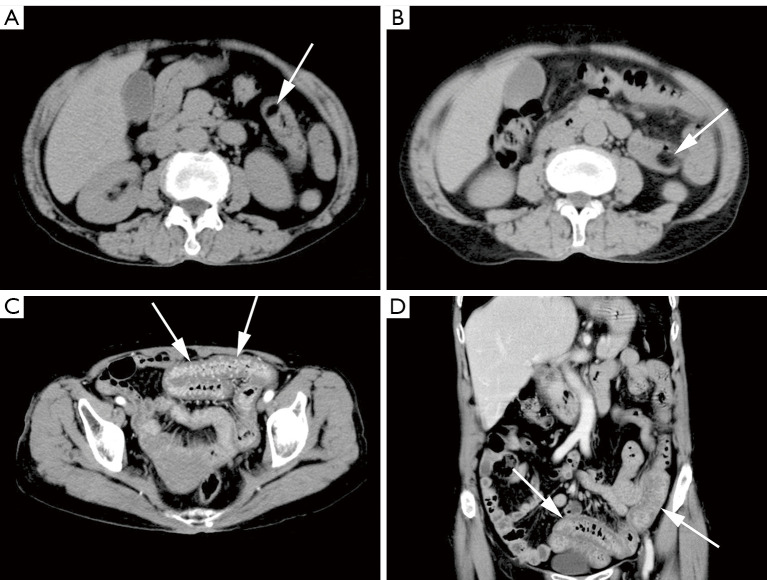
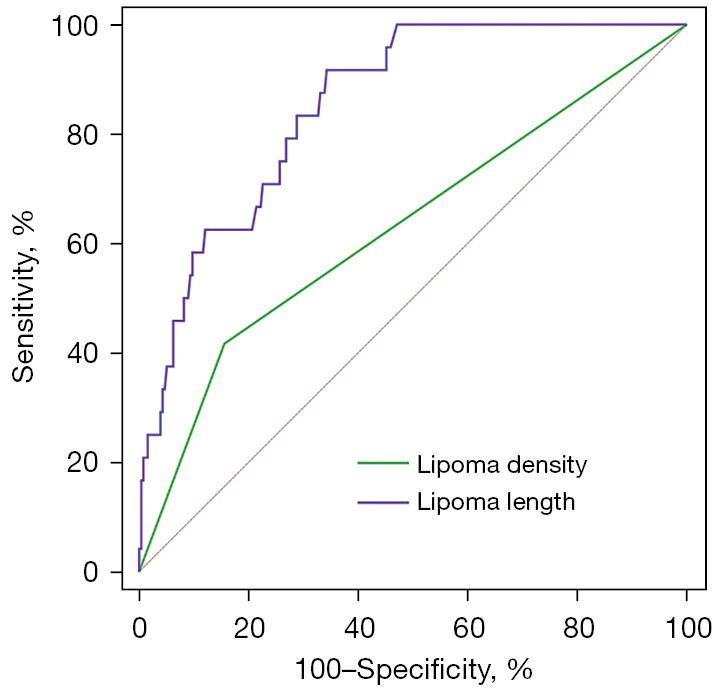
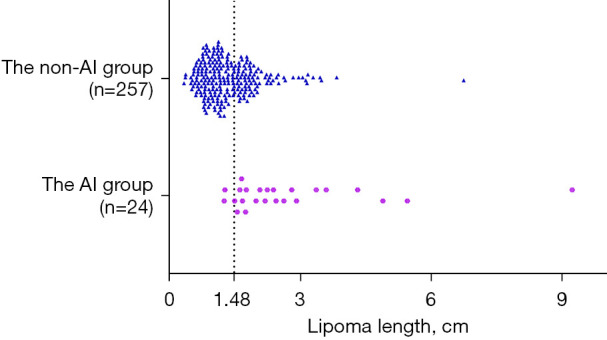
Results: A total of 281 patients with intestinal lipomas were included in the study, with an average age of 68.0±11.3 years, and the male to female ratio was about 1:1.4. Among them, 24 patients developed lipoma-induced intussusception. Patients in the AI group presented with more abdominal pain (70.8% vs. 47.1%, P=0.03), nausea/vomiting (37.5% vs. 14.8%, P=0.009), hematochezia/melena (29.2% vs. 11.3%, P=0.02), and abdominal tenderness (66.7% vs. 24.9%, P<0.001). Lipomas were more common in the small bowel (224/281, 79.7%) than the large bowel (57/281, 20.3%). Lipomas in the AI group showed more heterogeneous hypodensity (41.7% vs. 15.6%, P=0.004), longer length (median, 2.2 vs. 1.2 cm, P<0.001), and larger volume (median, 4.1 vs. 0.6 cm3, P<0.001). In the univariate logistic regression, lipoma density [odds ratio (OR) =3.875, 95% confidence interval (CI): 1.609-9.331, P=0.003] and lipoma length (OR =3.216, 95% CI: 1.977-5.231, P<0.001) were risk factors for intestinal lipoma-induced intussusception.
Conclusions: More patients in the AI group have digestive tract symptoms than those in the non-AI group. Lipoma density and length are risk factors for intussusception in patients with intestinal lipoma. In addition, the common site of intestinal lipoma may have changed from the colon to the small intestine.
Keywords: Lipoma; complications; intussusception; multidetector computed tomography (MDCT); risk factors.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1530/coif). The authors declare that the study was supported by the grant from the Clinical Medical Research Project of Army Medical University (No. 2022XLC08). The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Giant pedunculated colonic lipoma causing colo-colic intussusception in a patient with mechanical ileus.Ann Ital Chir. 2020 Mar 3;9:S2239253X20032296. Ann Ital Chir. 2020. PMID: 32989208
-
[Intestinal occlusion due to a colonic lipoma. Apropos 2 cases].Minerva Chir. 1993 Sep 30;48(18):1035-9. Minerva Chir. 1993. PMID: 8290148 Italian.
-
Intestinal intussusception related to colonic pedunculated lipoma: A case report and review of the literature.Int J Surg Case Rep. 2019;55:206-209. doi: 10.1016/j.ijscr.2019.01.042. Epub 2019 Feb 10. Int J Surg Case Rep. 2019. PMID: 30771623 Free PMC article.
-
[Intestinal invagination caused by colonic lipoma].Minerva Chir. 1996 Sep;51(9):717-23. Minerva Chir. 1996. PMID: 9082238 Review. Italian.
-
Adult ileoileal intussusception induced by an ileal lipoma diagnosed preoperatively: report of a case and review of the literature.Surg Today. 2012 Jul;42(7):686-92. doi: 10.1007/s00595-011-0092-6. Epub 2011 Dec 14. Surg Today. 2012. PMID: 22167483 Review.
References
-
- Mouaqit O, Hasnai H, Chbani L, Benjelloun B, El Bouhaddouti H, Ibn El Majdoub K, Toughrai I, Laalim SA, Oussaden A, Maazaz K, Amarti A, Taleb KA. Adult intussusceptions caused by a lipoma in the jejunum: report of a case and review of the literature. World J Emerg Surg 2012;7:28. 10.1186/1749-7922-7-28 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources