

Safety and efficacy of ultrasound-guided percutaneous flexor retinaculum release of the ankle: an anatomical study
- PMID: 38846301
- PMCID: PMC11151242
- DOI: 10.21037/qims-24-81
Safety and efficacy of ultrasound-guided percutaneous flexor retinaculum release of the ankle: an anatomical study
Abstract
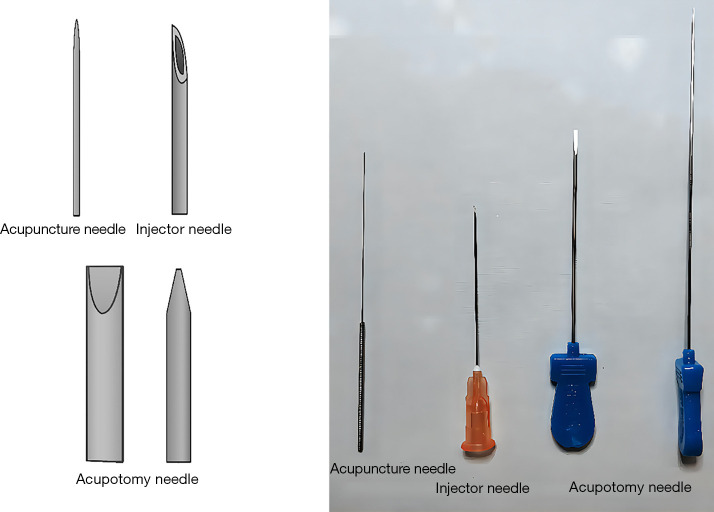
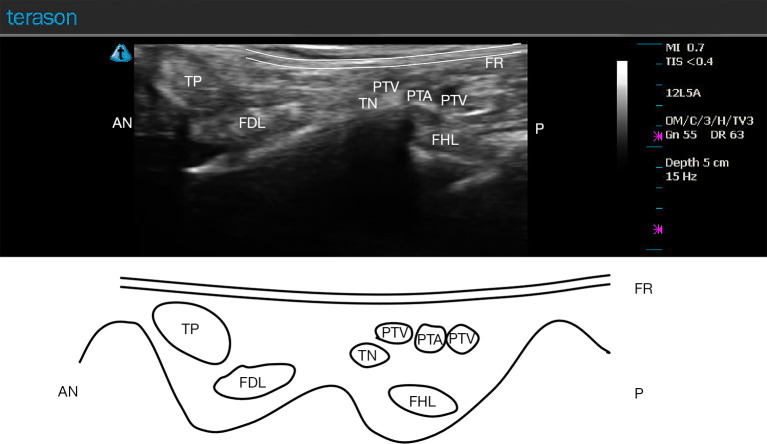
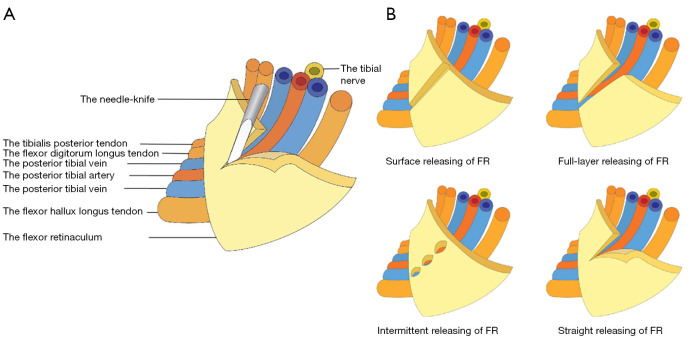
Background: Tarsal tunnel syndrome (TTS) is a condition in which the tibial nerve (TN) (or its terminal branches) is compressed by the flexor retinaculum (FR) and the deep fascia of the abductor hallucis muscle at the tarsal tunnel, causing symptoms that negatively impact the patient's quality of life, including numbness, a sensation of a foreign object, coldness, and pain. FR release via microtrauma using needle-knife has proven to be effective in China and is widely used by clinicians. The traditional acupotomy, however, is the "blind knife" treatment, which cannot guarantee patient safety due to risk of injury to important structures, particularly the neurovascular bundle. Compared with the conventional treatments, ultrasound-guided percutaneous FR release possesses noteworthy advantages including high efficacy and safety.
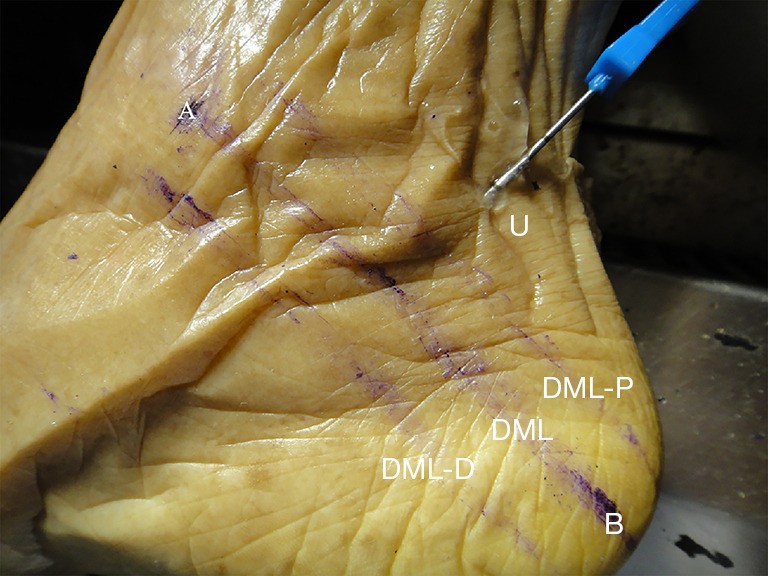
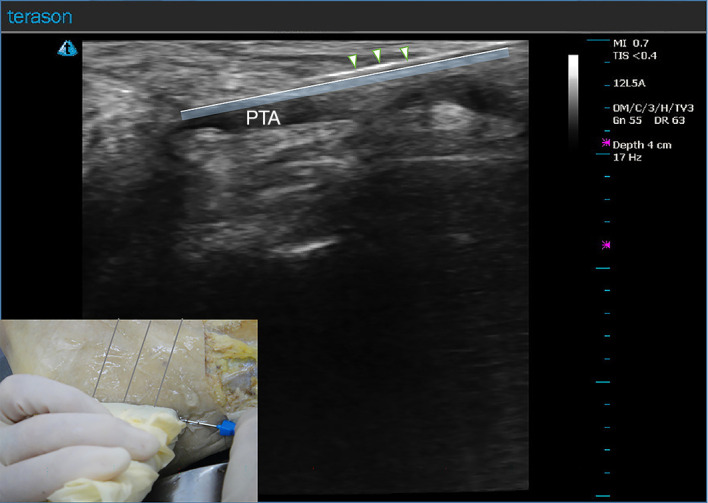
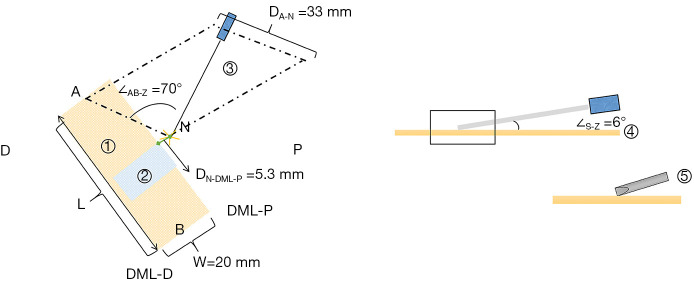
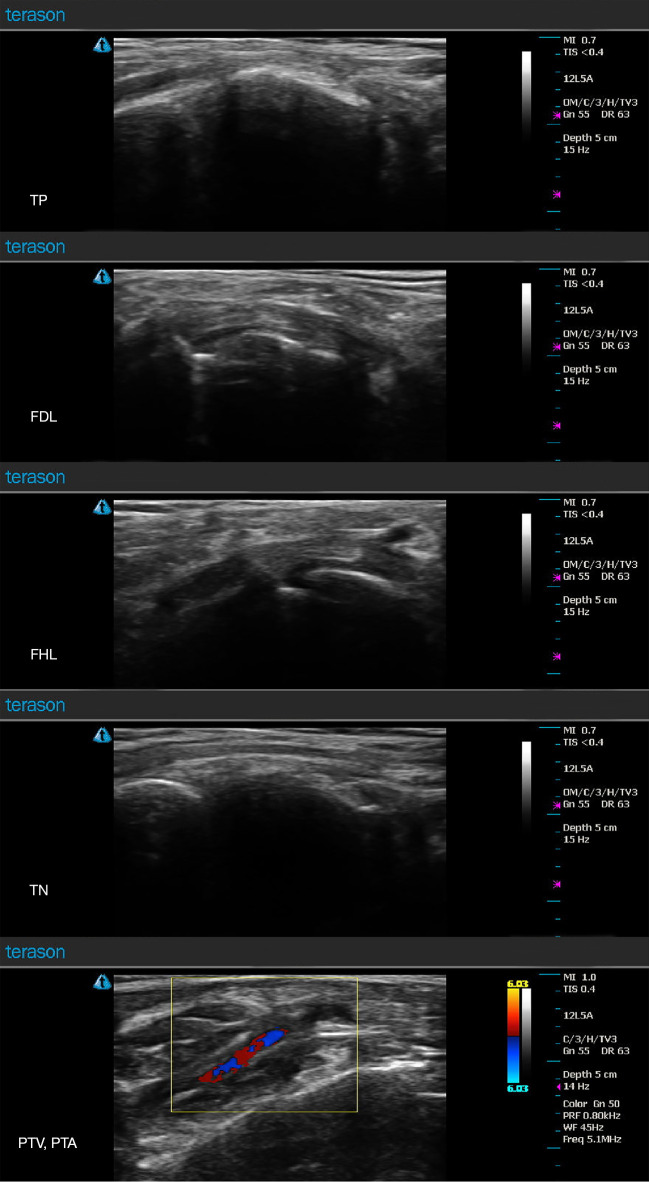
Methods: Percutaneous release of the FR was performed on 51 formalin-fixed specimens. The specimens were divided into two groups: an ultrasound-guided acupotomy pushing group comprising 20 legs (group U) and a nonultrasound-guided acupotomy pushing group comprising 31 legs (group N). After high-frequency ultrasound exploration, those with clear vascular imaging were included in group U; otherwise, they were included in group N. The FR was released percutaneously, soft tissue was dissected layer by layer, and anatomical data were recorded.
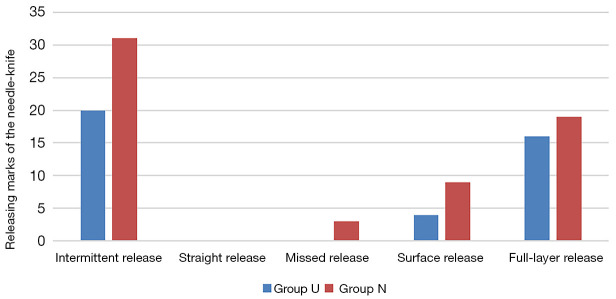
Results: There no cases of injury in group U (0%) and four in group N (12.9%). Among the different intervention methods, there were no significant differences in tissue injury types (χ2=2.80; P=0.09). The percentage of released FR in group U was 80.00% while that in group N was 61.29% (χ2=1.977; P=0.16), which did not represent a significant difference between the two groups. However, group U had a significantly greater release length than that in the group N (t=3.359; P=0.002), indicating that the flexor release length guided by ultrasound is significantly greater than the unguided one.
Conclusions: Ultrasound-guided percutaneous release of the FR using a needle-knife can provide greater length and percentage of released FR while maintaining a comparable safety rate to the unguided procedure.
Keywords: Acupotome; anatomy; percutaneous release; tarsal tunnel syndrome (TTS); ultrasound-guided technique.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-81/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
[Clinical anatomical study on the treatment of tarsal tunnel syndrome with four-point vertical acupotomy].Zhongguo Gu Shang. 2022 Jun 25;35(6):543-7. doi: 10.12200/j.issn.1003-0034.2022.06.008. Zhongguo Gu Shang. 2022. PMID: 35730224 Chinese.
-
Safety and efficacy of ultrasound-guided percutaneous A1 pulley release using a needle knife: An anatomical study.Front Surg. 2022 Sep 20;9:967400. doi: 10.3389/fsurg.2022.967400. eCollection 2022. Front Surg. 2022. PMID: 36204345 Free PMC article.
-
Ultrasound-Guided Percutaneous A1 Pulley Release by Acupotomy (Needle-Knife): A Cadaveric Study of Safety and Efficacy.J Pain Res. 2022 Feb 9;15:413-422. doi: 10.2147/JPR.S349869. eCollection 2022. J Pain Res. 2022. PMID: 35173479 Free PMC article.
-
Tarsal tunnel syndrome-A narrative literature review.Foot (Edinb). 2015 Dec;25(4):244-50. doi: 10.1016/j.foot.2015.08.008. Epub 2015 Sep 12. Foot (Edinb). 2015. PMID: 26546070 Review.
-
Ultrasound-Guided Surgery for Carpal Tunnel Syndrome: A New Interventional Procedure.Semin Intervent Radiol. 2018 Oct;35(4):248-254. doi: 10.1055/s-0038-1673360. Epub 2018 Nov 5. Semin Intervent Radiol. 2018. PMID: 30402007 Free PMC article. Review.
References
-
- Sun XJ, Shi C, Li YN, Lan YJ, Wang JW, Zhang WG, Li SL. Clinical anatomical study on the treatment of tarsal tunnel syndrome with four-point vertical acupotomy. Zhongguo Gu Shang 2022;35:543-7. - PubMed
LinkOut - more resources
Full Text Sources