

For older women, the majority of hip fragility fractures and radiographic vertebral fragility fractures occur among the densitometrically osteoporotic population: a literature analysis
- PMID: 38846307
- PMCID: PMC11151245
- DOI: 10.21037/qims-24-227
For older women, the majority of hip fragility fractures and radiographic vertebral fragility fractures occur among the densitometrically osteoporotic population: a literature analysis
Abstract
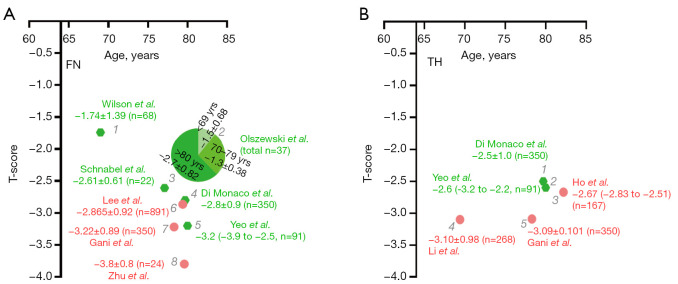
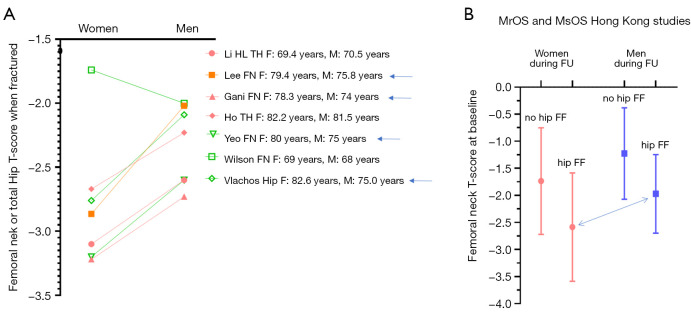
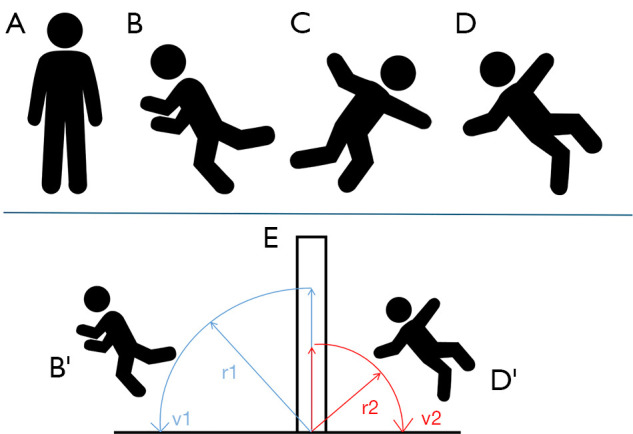
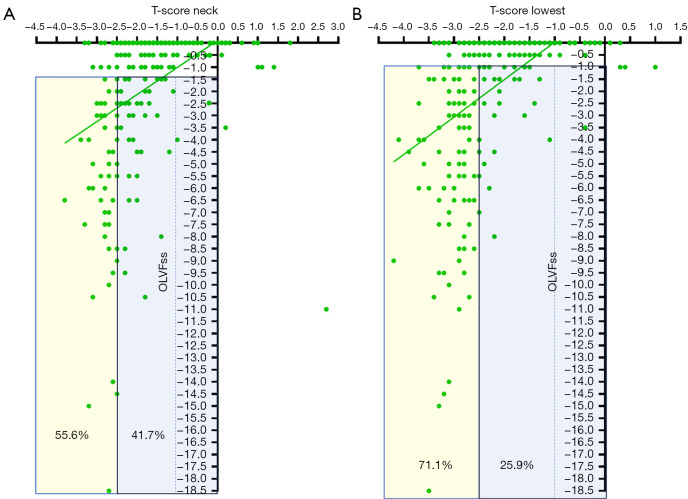
It has been frequently cited that 'the majority of fragility fractures (FF) occur at non-osteoporotic bone mineral density (BMD)'. For the reports with T-score measured around the time of a hip fracture, we conducted a systematic literature search in December 2022, and resulted in 10 studies with five for Caucasian women and five for East Asian women. Femoral neck (FN) T-score was reported in five Caucasian studies and three East Asian studies, three of five Caucasian studies had a mean T-score ≤-2.5, and one study had the majority of their patients measuring a mean T-score ≤-2.5. All three East Asian studies reported a mean FN T-score ≤-2.7. Total hip T-score was reported in two Caucasian studies and three East Asian studies, the two Caucasian studies both had a mean T-score ≤-2.5, and all three East Asian studies had a mean T-score ≤-2.6. A new literature search conducted in April 2024 results in additional three studies, with results being consistent with the data described above. A trend was noted that 'younger' patients suffer from hip fractures at a 'higher' T-score. For the highly cited articles where the notion the majority of FF occur at non-osteoporotic BMD was derived from, authors reported prospective epidemiological studies where BMD was not measured at the timepoint of hip fracture, instead, BMD was measured at the study baseline. These epidemiological studies suggest that >50% of hip fractures likely occur in women with an osteoporotic FN or hip T-score. However, a pattern was seen that older men suffer from hip fracture at a notably higher T-score than older women. For the cases of radiographic vertebral FF, despite varying criteria being used to classify these FFs, the majority of female patients had spine densitometric osteoporosis. Literature shows, compared with the cases of hip fracture, distal forearm fracture occurs at a 'younger' age and 'higher' BMD, suggesting distal forearm fracture is more likely associated with a 'higher' trauma energy level.
Keywords: Bone mineral density (BMD); hip fracture; osteoporosis; osteoporotic vertebral fracture; prevalence.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The author has completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-227/coif). Y.X.J.W. serves as the Editor-in-Chief of Quantitative Imaging in Medicine and Surgery. The author has no other conflicts of interest to declare.
Figures
Similar articles
-
Utilization of DXA Bone Mineral Densitometry in Ontario: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(20):1-180. Epub 2006 Nov 1. Ont Health Technol Assess Ser. 2006. PMID: 23074491 Free PMC article.
-
Revision of the 1994 World Health Organization T-score definition of osteoporosis for use in older East Asian women and men to reconcile it with their lifetime risk of fragility fracture.Skeletal Radiol. 2024 Apr;53(4):609-625. doi: 10.1007/s00256-023-04481-7. Epub 2023 Oct 27. Skeletal Radiol. 2024. PMID: 37889317 Review.
-
BMD T-score discriminates trochanteric fractures from unfractured controls, whereas geometry discriminates cervical fracture cases from unfractured controls of similar BMD.Osteoporos Int. 2010 Jul;21(7):1269-76. doi: 10.1007/s00198-009-1070-3. Epub 2009 Sep 26. Osteoporos Int. 2010. PMID: 19784537
-
Bone mineral density and trabecular bone score in elderly type 2 diabetes Southeast Asian patients with severe osteoporotic hip fractures.PLoS One. 2020 Nov 19;15(11):e0241616. doi: 10.1371/journal.pone.0241616. eCollection 2020. PLoS One. 2020. PMID: 33211723 Free PMC article.
-
Osteoporosis: assessing the risk of fragility fracture.London: National Institute for Health and Care Excellence (NICE); 2017 Feb. London: National Institute for Health and Care Excellence (NICE); 2017 Feb. PMID: 32186835 Free Books & Documents. Review.
Cited by
-
Construction and validation of a nomogram prediction model for the need for intensive care unit admission after hip fracture surgery.Medicine (Baltimore). 2025 Jun 13;104(24):e42793. doi: 10.1097/MD.0000000000042793. Medicine (Baltimore). 2025. PMID: 40527820 Free PMC article.
-
Osteopenic fractures, the importance of applying gender-specific bone mineral density thresholds in identifying hip fracture at-risk populations, and comments on the article of Xu et al.Quant Imaging Med Surg. 2025 Jan 2;15(1):1094-1100. doi: 10.21037/qims-24-2379. Epub 2024 Nov 25. Quant Imaging Med Surg. 2025. PMID: 39839021 Free PMC article. No abstract available.
-
The observation that older men suffer from hip fracture at DXA T-scores higher than older women and a proposal of a new low BMD category, osteofrailia, for predicting fracture risk in older men.Skeletal Radiol. 2025 May;54(5):925-936. doi: 10.1007/s00256-024-04793-2. Epub 2024 Sep 16. Skeletal Radiol. 2025. PMID: 39284928 Free PMC article.
-
Majority of hip fragility fractures among older people can be predicted by a DXA examination: an updated analysis of literature results and empirical Chinese data with a focus on the validation of the newly proposed osteofrailia criterion for men.Quant Imaging Med Surg. 2025 Jan 2;15(1):473-485. doi: 10.21037/qims-2024-2568. Epub 2024 Dec 17. Quant Imaging Med Surg. 2025. PMID: 39839001 Free PMC article.
References
-
- Brown SE. What a diagnosis of osteopenia means for you. Available online: https://www.betterbones.com/osteopenia/about-osteopenia/
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous