

Automated detection and classification of coronary atherosclerotic plaques on coronary CT angiography using deep learning algorithm
- PMID: 38846308
- PMCID: PMC11151262
- DOI: 10.21037/qims-23-1513
Automated detection and classification of coronary atherosclerotic plaques on coronary CT angiography using deep learning algorithm
Abstract
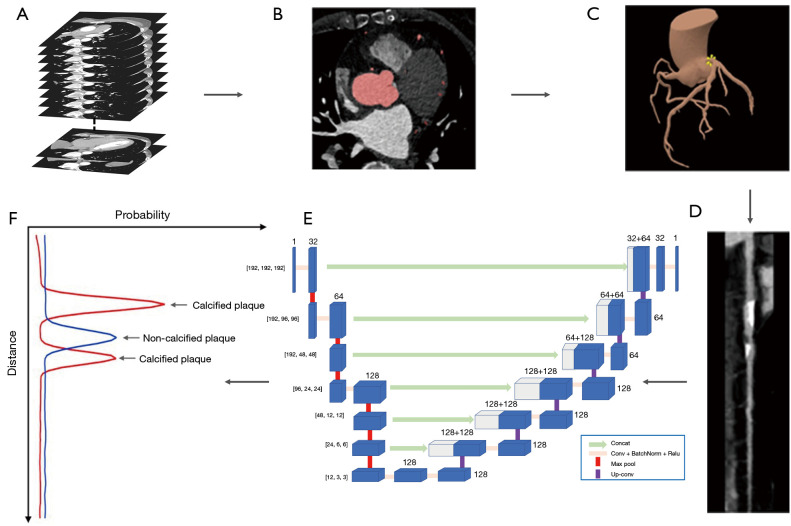
Background: Coronary artery disease (CAD) is the leading cause of mortality worldwide. Recent advances in deep learning technology promise better diagnosis of CAD and improve assessment of CAD plaque buildup. The purpose of this study is to assess the performance of a deep learning algorithm in detecting and classifying coronary atherosclerotic plaques in coronary computed tomographic angiography (CCTA) images.
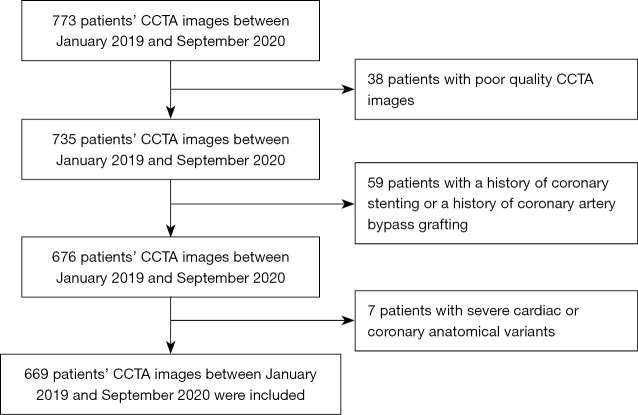
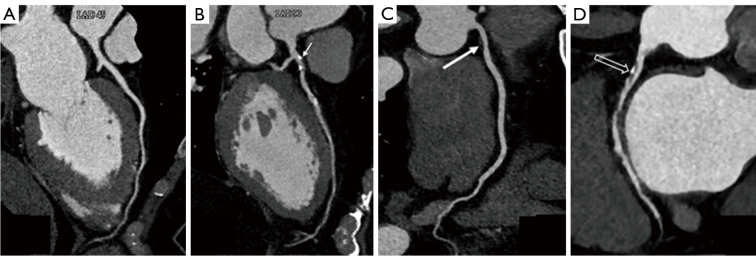
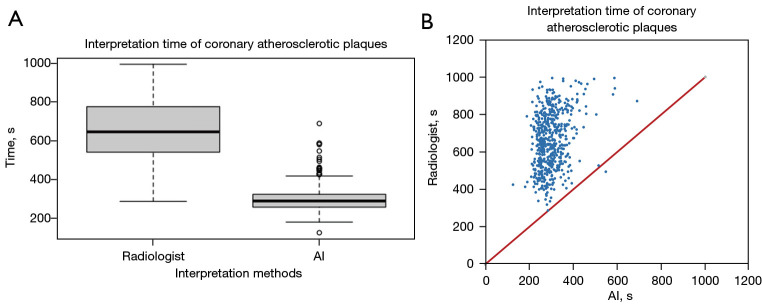
Methods: Between January 2019 and September 2020, CCTA images of 669 consecutive patients with suspected CAD from Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine were included in this study. There were 106 patients included in the retrospective plaque detection analysis, which was evaluated by a deep learning algorithm and four independent physicians with varying clinical experience. Additionally, 563 patients were included in the analysis for plaque classification using the deep learning algorithm, and their results were compared with those of expert radiologists. Plaques were categorized as absent, calcified, non-calcified, or mixed.
Results: The deep learning algorithm exhibited higher sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy {92% [95% confidence interval (CI): 89.5-94.1%], 87% (95% CI: 84.2-88.5%), 79% (95% CI: 76.1-82.4%), 95% (95% CI: 93.4-96.3%), and 89% (95% CI: 86.9-90.0%)} compared to physicians with ≤5 years of clinical experience in CAD diagnosis for the detection of coronary plaques. The algorithm's overall sensitivity, specificity, PPV, NPV, accuracy, and Cohen's kappa for plaque classification were 94% (95% CI: 92.3-94.7%), 90% (95% CI: 88.8-90.3%), 70% (95% CI: 68.3-72.1%), 98% (95% CI: 97.8-98.5%), 90% (95% CI: 89.8-91.1%) and 0.74 (95% CI: 0.70-0.78), indicating strong performance.
Conclusions: The deep learning algorithm has demonstrated reliable and accurate detection and classification of coronary atherosclerotic plaques in CCTA images. It holds the potential to enhance the diagnostic capabilities of junior radiologists and junior intervention cardiologists in the CAD diagnosis, as well as to streamline the triage of patients with acute coronary symptoms.
Keywords: Coronary computed tomographic angiography (CCTA); atherosclerotic plaques; coronary artery disease (CAD); deep learning.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1513/coif). Z.S. and X.C. are employees of Philips Healthcare. C.Z. is an employee of Shukun (Beijing) Network Technology. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Deep learning analysis in coronary computed tomographic angiography imaging for the assessment of patients with coronary artery stenosis.Comput Methods Programs Biomed. 2020 Nov;196:105651. doi: 10.1016/j.cmpb.2020.105651. Epub 2020 Jul 9. Comput Methods Programs Biomed. 2020. PMID: 32712571
-
Relationship of coronary artery plaque composition to coronary artery stenosis severity: results from the prospective multicenter ACCURACY trial.Atherosclerosis. 2011 Dec;219(2):573-8. doi: 10.1016/j.atherosclerosis.2011.05.032. Epub 2011 May 31. Atherosclerosis. 2011. PMID: 21696739 Clinical Trial.
-
[Value of fractional flow reserve derived from coronary computed tomographic angiography and plaque quantitative analysis in predicting adverse outcomes of non-obstructive coronary heart disease].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Jun;35(6):615-619. doi: 10.3760/cma.j.cn121430-20230215-00092. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37366128 Chinese.
-
The Role of Artificial Intelligence in Healthcare: Enhancing Coronary Computed Tomography Angiography for Coronary Artery Disease Management.Cureus. 2024 Jun 2;16(6):e61523. doi: 10.7759/cureus.61523. eCollection 2024 Jun. Cureus. 2024. PMID: 38957241 Free PMC article. Review.
-
Cardiac CT: atherosclerosis to acute coronary syndrome.Cardiovasc Diagn Ther. 2014 Dec;4(6):430-48. doi: 10.3978/j.issn.2223-3652.2014.11.03. Cardiovasc Diagn Ther. 2014. PMID: 25610801 Free PMC article. Review.
Cited by
-
Association between coronary plaque vulnerability features and multiparametric pericoronary fat indices on coronary computed tomography angiography: a cross-sectional study.Quant Imaging Med Surg. 2025 Aug 1;15(8):6897-6909. doi: 10.21037/qims-24-1002. Epub 2025 Jul 28. Quant Imaging Med Surg. 2025. PMID: 40785932 Free PMC article.
References
-
- Cappelletti A, Latib A, Mazzavillani M, Magni V, Calori G, Colombo A, Margonato A; Coronary Artery risk factors Profile and Prognostic localization (CAPP) Study. Severity and prognostic localization of critical coronary artery stenoses: correlation with clinical control of major traditional risk factors. Coron Artery Dis 2012;23:455-9. 10.1097/MCA.0b013e32835878c3 - DOI - PubMed
-
- Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, Naruse H, Ishii J, Hishida H, Wong ND, Virmani R, Kondo T, Ozaki Y, Narula J. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol 2009;54:49-57. 10.1016/j.jacc.2009.02.068 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous