

Effectiveness of glucose-lowering medications on cardiovascular outcomes in patients with type 2 diabetes at moderate cardiovascular risk
- PMID: 38846711
- PMCID: PMC11156225
- DOI: 10.1038/s44161-024-00453-9
Effectiveness of glucose-lowering medications on cardiovascular outcomes in patients with type 2 diabetes at moderate cardiovascular risk
Abstract
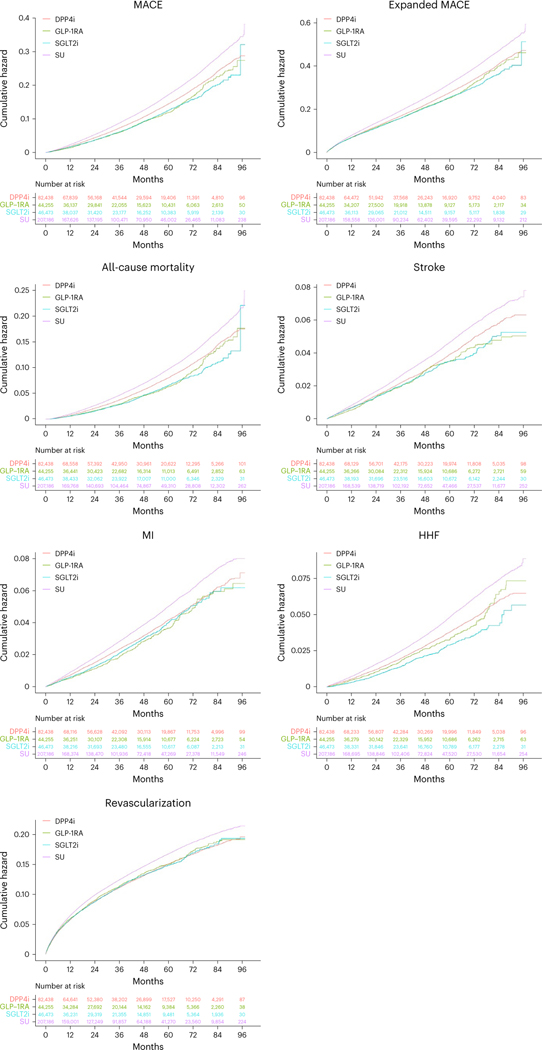
Cardiovascular disease (CVD) is the leading cause of death among people with type 2 diabetes1-5, most of whom are at moderate CVD risk6, yet there is limited evidence on the preferred choice of glucose-lowering medication for CVD risk reduction in this population. Here, we report the results of a retrospective cohort study where data for US adults with type 2 diabetes and moderate risk for CVD are used to compare the risks of experiencing a major adverse cardiovascular event with initiation of glucagon-like peptide-1 receptor agonists (GLP-1RA; n = 44,188), sodium-glucose cotransporter 2 inhibitors (SGLT2i; n = 47,094), dipeptidyl peptidase-4 inhibitors (DPP4i; n = 84,315) and sulfonylureas (n = 210,679). Compared to DPP4i, GLP-1RA (hazard ratio (HR) 0.87; 95% confidence interval (CI) 0.82-0.93) and SGLT2i (HR 0.85; 95% CI 0.81-0.90) were associated with a lower risk of a major adverse cardiovascular event, whereas sulfonylureas were associated with a higher risk (HR 1.19; 95% CI 1.16-1.22). Thus, GLP-1RA and SGLT2i may be the preferred glucose-lowering agents for cardiovascular risk reduction in patients at moderate baseline risk for CVD. ClinicalTrials.gov registration: NCT05214573.
Figures
References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical