

Exosomal ROR1 in peritoneal fluid identifies peritoneal disseminated PDAC and is associated with poor survival
- PMID: 38846943
- PMCID: PMC11153717
- DOI: 10.3389/fimmu.2024.1253072
Exosomal ROR1 in peritoneal fluid identifies peritoneal disseminated PDAC and is associated with poor survival
Abstract
Background: Pancreatic ductal adenocarcinoma (PDAC) is one of the deadliest forms of cancer and peritoneal dissemination is one major cause for this poor prognosis. Exosomes have emerged as promising biomarkers for gastrointestinal cancers and can be found in all kinds of bodily fluids, also in peritoneal fluid (PF). This is a unique sample due to its closeness to gastrointestinal malignancies. The receptor tyrosine kinase-like orphan receptor 1 (ROR1) has been identified as a potential biomarker in human cancers and represents a promising target for an immunotherapy approach, which could be considered for future treatment strategies. Here we prospectively analyzed the exosomal surface protein ROR1 (exo-ROR1) in PF in localized PDAC patients (PER-) on the one hand and peritoneal disseminated tumor stages (PER+) on the other hand followed by the correlation of exo-ROR1 with clinical-pathological parameters.
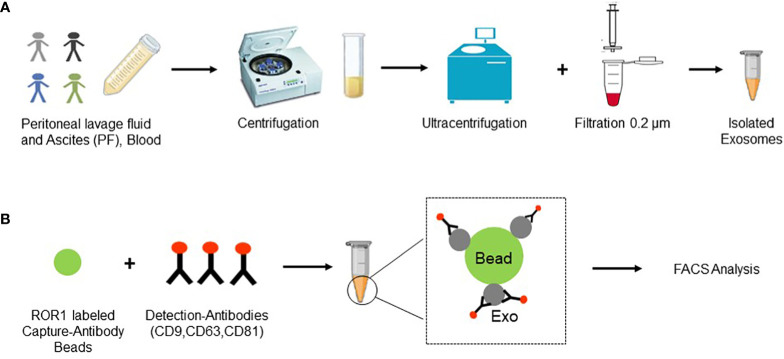
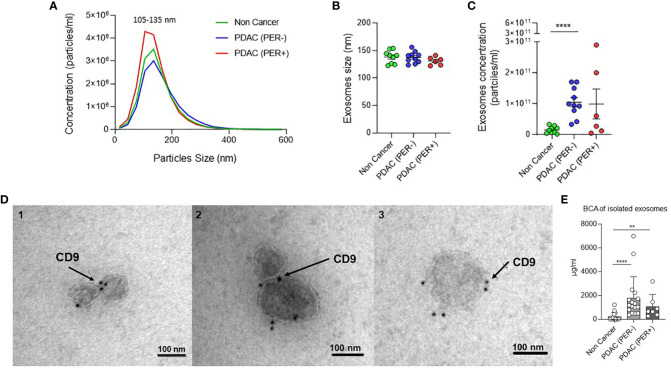
Methods: Exosomes were isolated from PF and plasma samples of non-cancerous (NC) (n = 15), chronic pancreatitis (CP) (n = 4), localized PDAC (PER-) (n = 18) and peritoneal disseminated PDAC (PER+) (n = 9) patients and the surface protein ROR1 was detected via FACS analysis. Additionally, soluble ROR1 in PF was analyzed. ROR1 expression in tissue was investigated using western blots (WB), qPCR, and immunohistochemistry (IHC). Exosome isolation was proven by Nano Tracking Analysis (NTA), WB, Transmission electron microscopy (TEM), and BCA protein assay. The results were correlated with clinical data and survival analysis was performed.
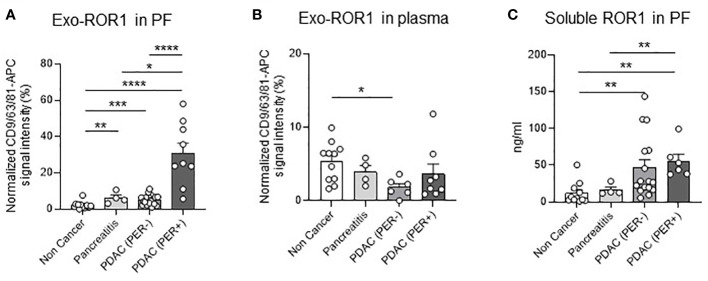
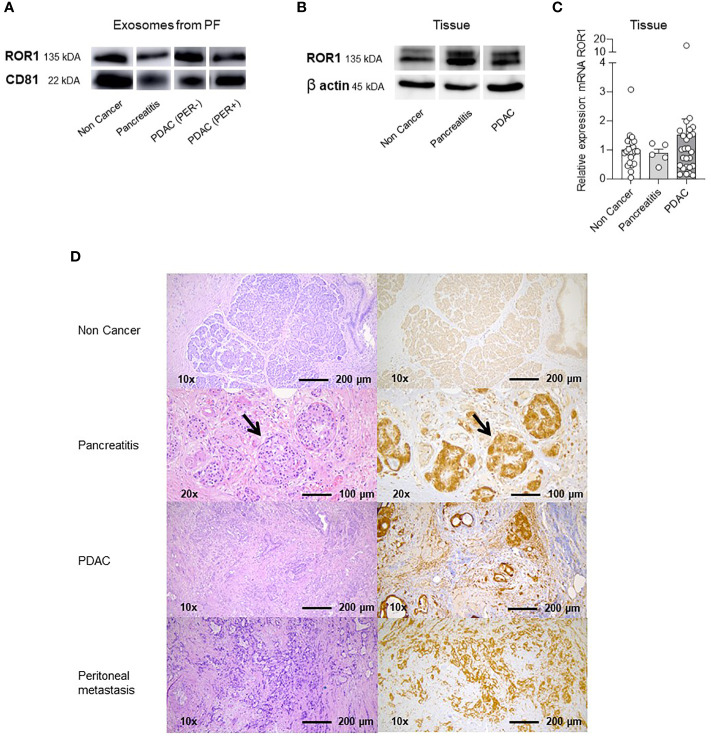
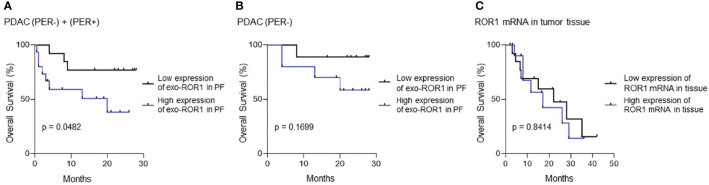
Results: PDAC (PER+) patients have the highest exo-ROR1 values in PF and can be discriminated from NC (p <0.0001), PDAC (PER-) (p <0.0001), and CP (p = 0.0112). PDAC (PER-) can be discriminated from NC (p = 0.0003). In plasma, exo-ROR1 is not able to distinguish between the groups. While there is no expression of ROR1 in the exocrine pancreatic tissue, PDAC and peritoneal metastasis show expression of ROR1. High exo-ROR1 expression in PF is associated with lower overall survival (p = 0.0482).
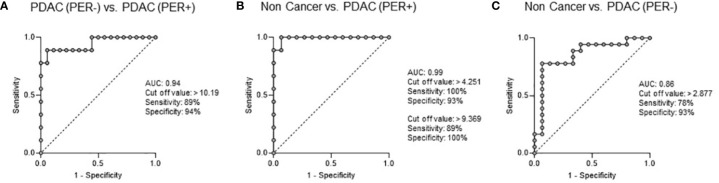
Conclusion: With exo-ROR1 in PF we found a promising diagnostic and prognostic biomarker possibly discriminating between NC, PDAC (PER-) and PDAC (PER+) and might shed light on future diagnostic and therapeutic concepts in PDAC.
Keywords: PDAC; ROR1; biomarker; exosomes; peritoneal carcinomatosis; peritoneal fluid; peritoneal lavage; targeted therapy.
Copyright © 2024 Mittelstädt, Anthuber, David, Podolska, Bénard, Brunner, Krautz, Jacobsen, Denz, Weber, Merkel, Hackner, Buniatov, Roßdeutsch, Klösch, Swierzy, Hansen, Strobel, Zopf, Baur, Van Deun, Immanuel Geppert, Gießl, Lettmaier, Semrau, Grützmann, Kouhestani and Weber.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Suenaga M, Fujii T, Kanda M, Takami H, Okumura N, Inokawa Y, et al. Pattern of first recurrent lesions in pancreatic cancer: hepatic relapse is associated with dismal prognosis and portal vein invasion. Hepatogastroenterol. (2014) 61:1756–61. - PubMed
-
- Jones RP, Psarelli E-E, Jackson R, Ghaneh P, Halloran CM, Palmer DH, et al. Patterns of recurrence after resection of pancreatic ductal adenocarcinoma: A secondary analysis of the ESPAC-4 randomized adjuvant chemotherapy trial. JAMA Surgery. (2019) 154:1038–48. doi: 10.1001/jamasurg.2019.3337 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous