

Diagnostic Strategies in Pulmonary Embolism
- PMID: 38846998
- PMCID: PMC11152624
- DOI: 10.1055/s-0044-1779661
Diagnostic Strategies in Pulmonary Embolism
Abstract
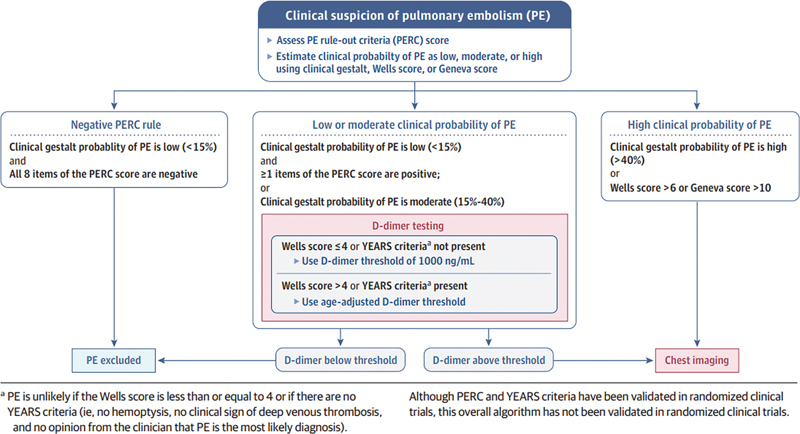
Key to the diagnosis of pulmonary embolism (PE) is a careful bedside evaluation. After this, there are three further diagnostic steps. In all patients, estimation of the clinical probability of PE is performed. The other two steps are measurement of D-dimer when indicated and chest imaging when indicated. The clinical probability of PE is estimated at low, moderate, or high. The prevalence of PE is less than 15% among patients with low clinical probability, 15 to 40% with moderate clinical probability, and >40% in patients with high clinical probability. Clinical gestalt has been found to be very useful in estimating probability of PE. However, clinical prediction rules, such as Wells criteria, the modified Geneva score, and the PE rule out criteria have been advocated as adjuncts. In patients with high clinical probability, the high prevalence of PE can lower the D-dimer negative predictive value, which could increase the risk of diagnostic failure. Consequently, patients with high probability for PE need to proceed directly to chest imaging, without prior measurement of D-dimer level. Key studies in determining which low to moderate probability patients require chest imaging are the Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism (ADJUST-PE), the Simplified diagnostic management of suspected pulmonary embolism (YEARS), and the Pulmonary Embolism Graduated D-Dimer trials. In patients with low clinical probability, PE can be excluded without imaging studies if D-dimer is less than 1,000 ng/mL. In patients in whom there is not a low likelihood for PE, this can be excluded without imaging studies if the D-dimer is below the age-adjusted threshold.
Keywords: Geneva score; PERC Rule; Wells criteria; YEARS algorithm; diagnostic strategies; gestalt; pulmonary embolism.
International College of Angiology. This article is published by Thieme.
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
The Legend score synthesizes Wells, PERC, Geneva, D-dimer and predicts acute pulmonary embolism prior to imaging tests.Pulmonology. 2025 Dec 31;31(1):2416828. doi: 10.1016/j.pulmoe.2023.10.002. Epub 2024 Oct 24. Pulmonology. 2025. PMID: 37953212
-
Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study.JAMA. 2014 Mar 19;311(11):1117-24. doi: 10.1001/jama.2014.2135. JAMA. 2014. PMID: 24643601
-
Retrospective validation of the pulmonary embolism rule-out criteria rule in 'PE unlikely' patients with suspected pulmonary embolism.Eur J Emerg Med. 2018 Jun;25(3):185-190. doi: 10.1097/MEJ.0000000000000442. Eur J Emerg Med. 2018. PMID: 28002070
-
Clinical decision rules for excluding pulmonary embolism: a meta-analysis.Ann Intern Med. 2011 Oct 4;155(7):448-60. doi: 10.7326/0003-4819-155-7-201110040-00007. Ann Intern Med. 2011. PMID: 21969343 Review.
-
Diagnosis and Exclusion of Pulmonary Embolism.Thromb Res. 2018 Mar;163:207-220. doi: 10.1016/j.thromres.2017.06.002. Epub 2017 Jun 7. Thromb Res. 2018. PMID: 28683951 Review.
Cited by
-
A Comparative Analysis of the Impact of Severe Acute Respiratory Syndrome Coronavirus 2 Infection on the Performance of Clinical Decision-Making Algorithms for Pulmonary Embolism.J Clin Med. 2024 Nov 21;13(23):7008. doi: 10.3390/jcm13237008. J Clin Med. 2024. PMID: 39685466 Free PMC article.
References
-
- Freund Y, Cohen-Aubart F, Bloom B. Acute pulmonary embolism: a review. JAMA. 2022;328(13):1336–1345. - PubMed
-
- Duffett L, Castellucci L A, Forgie M A. Pulmonary embolism: update on management and controversies. BMJ. 2020;370:m2177. - PubMed
-
- Hampson N B, Culver B H. Clinical aspects of pulmonary embolism. Semin Ultrasound CT MR. 1997;18(05):314–322. - PubMed
-
- Huisman M V, Barco S, Cannegieter S C et al.Pulmonary embolism. Nat Rev Dis Primers. 2018;4:18028. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
