

Office measurement vs. ambulatory blood pressure monitoring: associations with mortality in patients with or without diabetes
- PMID: 38847237
- PMCID: PMC11328865
- DOI: 10.1093/eurheartj/ehae337
Office measurement vs. ambulatory blood pressure monitoring: associations with mortality in patients with or without diabetes
Abstract
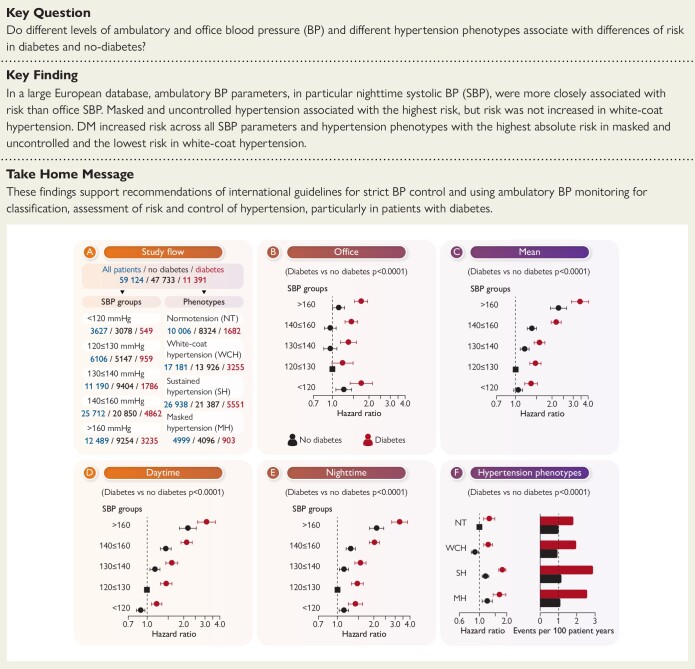
Background and aims: Guidelines suggest similar blood pressure (BP) targets in patients with and without diabetes and recommend ambulatory BP monitoring (ABPM) to diagnose and classify hypertension. It was explored whether different levels of ambulatory and office BP and different hypertension phenotypes associate with differences of risk in diabetes and no diabetes.
Methods: This analysis assessed outcome data from the Spanish ABPM Registry in 59 124 patients with complete available data. The associations between office, mean, daytime, and nighttime ambulatory BP with the risk in patients with or without diabetes were explored. The effects of diabetes on mortality in different hypertension phenotypes, i.e. sustained hypertension, white-coat hypertension, and masked hypertension, compared with normotension were studied. Analyses were done with Cox regression analyses and adjusted for demographic and clinical confounders.
Results: A total of 59 124 patients were recruited from 223 primary care centres in Spain. The majority had an office systolic BP >140 mmHg (36 700 patients), and 23 128 (40.6%) patients were untreated. Diabetes was diagnosed in 11 391 patients (19.2%). Concomitant cardiovascular (CV) disease was present in 2521 patients (23.1%) with diabetes and 4616 (10.0%) without diabetes. Twenty-four-hour mean, daytime, and nighttime ambulatory BP were associated with increased risk in diabetes and no diabetes, while in office BP, there was no clear association with no differences with and without diabetes. While the relative association of BP to CV death risk was similar in diabetes compared with no diabetes (mean interaction P = .80, daytime interaction P = .97, and nighttime interaction P = .32), increased event rates occurred in diabetes for all ABPM parameters for CV death and all-cause death. White-coat hypertension was not associated with risk for CV death (hazard ratio 0.86; 95% confidence interval 0.72-1.03) and slightly reduced risk for all-cause death in no diabetes (hazard ratio 0.89; confidence interval 0.81-0.98) but without significant interaction between diabetes and no diabetes. Sustained hypertension and masked hypertension in diabetes and no diabetes were associated with even higher risk. There were no significant interactions in hypertensive phenotypes between diabetes and no diabetes and CV death risk (interaction P = .26), while some interaction was present for all-cause death (interaction P = .043) and non-CV death (interaction P = .053).
Conclusions: Diabetes increased the risk for all-cause death, CV, and non-CV death at every level of office and ambulatory BP. Masked and sustained hypertension confer to the highest risk, while white-coat hypertension appears grossly neutral without interaction of relative risk between diabetes and no diabetes. These results support recommendations of international guidelines for strict BP control and using ABPM for classification and assessment of risk and control of hypertension, particularly in patients with diabetes.
Clinical trial registration: Not applicable.
Keywords: Ambulatory blood pressure monitoring; Cardiovascular death; Diabetes; Hypertension.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Figures




References
-
- Perreault L, Pan Q, Aroda VR, Barrett-Connor E, Dabelea D, Dagogo-Jack S, et al. Diabetes Prevention Program Research Group. Exploring residual risk for diabetes and microvascular disease in the Diabetes Prevention Program Outcomes Study (DPPOS). Diabet Med 2017;34:1747–55. 10.1111/dme.13453 - DOI - PMC - PubMed
-
- Aroda VR, Knowler WC, Crandall JP, Perreault L, Edelstein SL, Jeffries SL, et al. Diabetes Prevention Program Research Group. Metformin for diabetes prevention: insights gained from the Diabetes Prevention Program/Diabetes Prevention Program Outcomes Study. Diabetologia 2017;60:1601–11. 10.1007/s00125-017-4361-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
