

Effect of different anesthetic modalities on postoperative delirium in elderly hip fractures: A meta-analysis
- PMID: 38847680
- PMCID: PMC11155603
- DOI: 10.1097/MD.0000000000038418
Effect of different anesthetic modalities on postoperative delirium in elderly hip fractures: A meta-analysis
Abstract
Background: Previous findings on the effect of general versus spinal anesthesia on postoperative delirium in elderly people with hip fractures are somewhat controversial. This article included the latest randomized controlled study for meta-analysis to evaluate the effect of general anesthesia (GA) and spinal anesthesia (SA) on delirium after hip fracture surgery in the elderly, so as to guide the clinical.
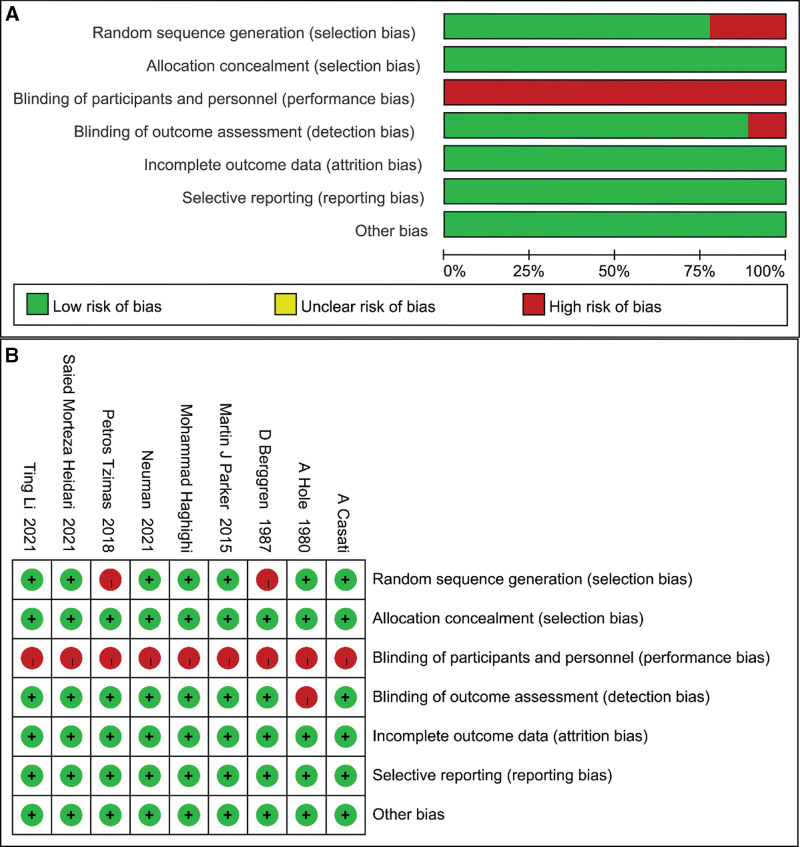
Methods: Cochrane Library, PubMed, Web Of Science, and Embase were searched from inception up to January 16, 2024. Randomized controlled trial (RCT) was included to evaluate the postoperative results of GA and SA in elderly patients (≥50 years old) undergoing hip fracture surgery. Two researchers independently screened for inclusion in the study and extracted data. Heterogeneity was assessed by the I²and Chi-square tests, and P < .1 or I² ≥ 50% indicated marked heterogeneity among studies. The Mantel-Haenszel method was used to estimate the combined relative risk ratio (RR) and the corresponding 95% confidence interval (CI) for the binary variables.
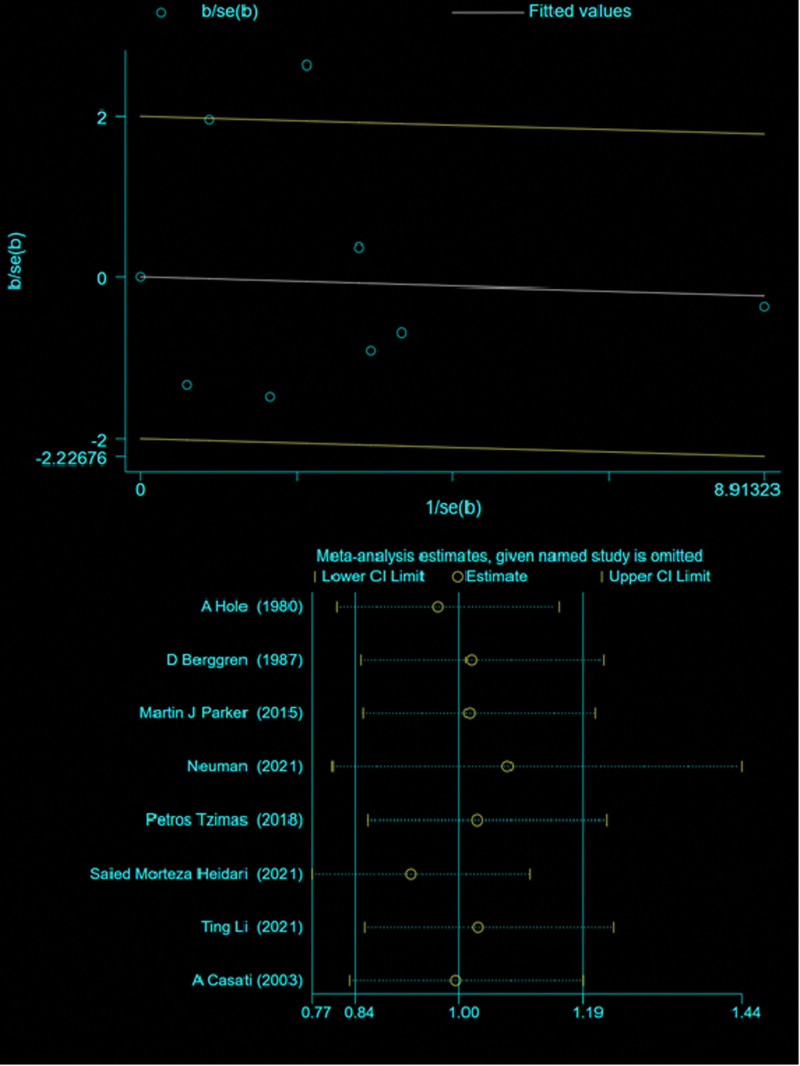
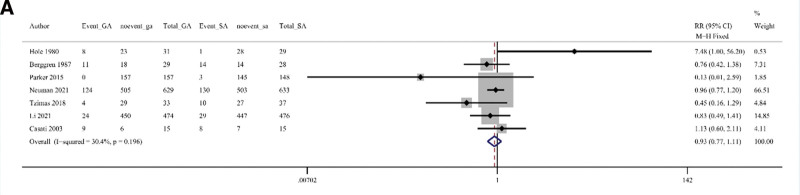
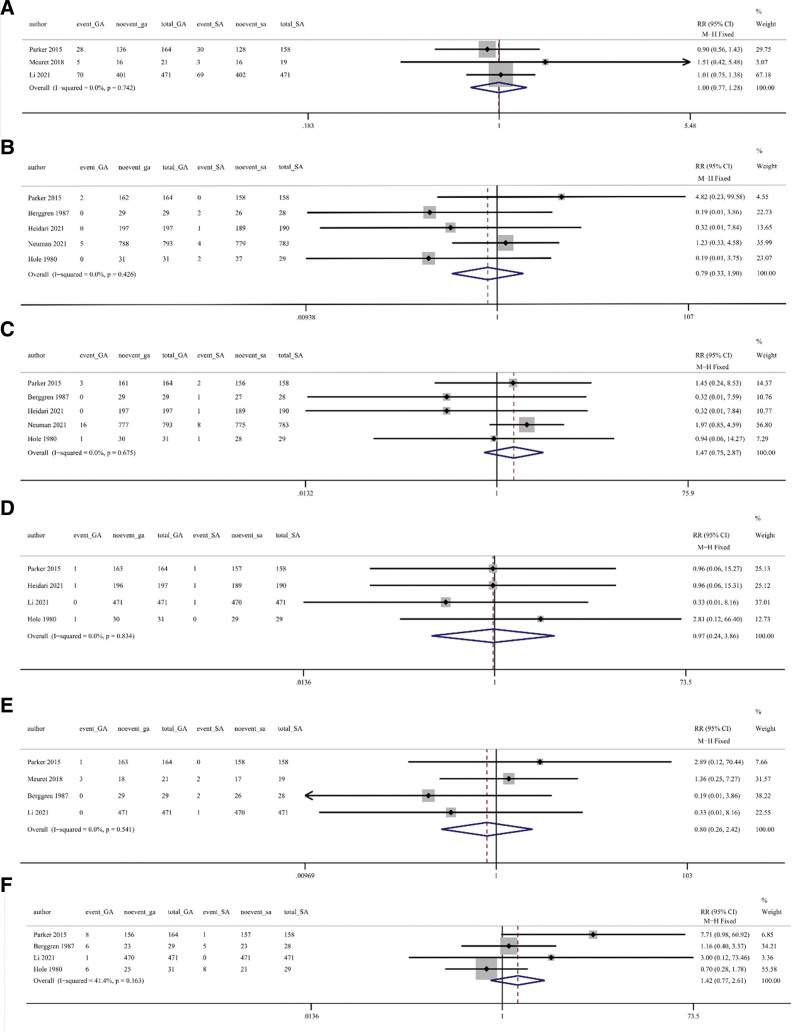
Results: Nine randomized controlled trials were included. There was no significant difference (RR = 0.93, 95% CI = 0.774-1.111, P > .05) in the incidence of postoperative delirium between the GA group and the SA group. In intraoperative blood transfusion (RR = 1.0, 95% CI = 0.77-1.28, Z = 0.04, P = .971), pulmonary embolism (RR = 0.795, 95% CI = 0.332-1.904, Z = 0.59, P = .606), pneumonia (RR = 1.47, 95% CI = 0.75-2.87, P = .675), myocardial infarction (RR = 0.97, 95% CI = 0.24-3.86, Z = 0.05, P = .961), heart failure (RR = 0.80, 95% CI = 0.26-2.42, Z = 0.40, P = .961), urinary retention (RR = 1.42, 95% CI = 0.77-2.61, Z = 1.11, P = .267) were similar between the 2 anesthetic techniques.
Conclusion: There is no significant difference in the effect of GA and SA on postoperative delirium in elderly patients with hip fracture, and their effects on postoperative complications are similar.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


Similar articles
-
Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial.JAMA. 2022 Jan 4;327(1):50-58. doi: 10.1001/jama.2021.22647. JAMA. 2022. PMID: 34928310 Free PMC article. Clinical Trial.
-
Neuraxial versus general anesthesia in elderly patients undergoing hip fracture surgery and the incidence of postoperative delirium: a systematic review and stratified meta-analysis.BMC Anesthesiol. 2023 Jul 22;23(1):250. doi: 10.1186/s12871-023-02196-9. BMC Anesthesiol. 2023. PMID: 37481517 Free PMC article.
-
Effects of general versus subarachnoid anaesthesia on circadian melatonin rhythm and postoperative delirium in elderly patients undergoing hip fracture surgery: A prospective cohort clinical trial.EBioMedicine. 2021 Aug;70:103490. doi: 10.1016/j.ebiom.2021.103490. Epub 2021 Jul 17. EBioMedicine. 2021. PMID: 34280784 Free PMC article.
-
Comparative efficacy of Neuraxial and general anesthesia for hip fracture surgery: a meta-analysis of randomized clinical trials.BMC Anesthesiol. 2020 Jun 30;20(1):162. doi: 10.1186/s12871-020-01074-y. BMC Anesthesiol. 2020. PMID: 32605591 Free PMC article.
-
Comparing the Effect of Spinal and General Anesthesia for Hip Fracture Surgery in Older Patients: A Meta-analysis of Randomized Clinical Trials.Orthop Surg. 2023 Dec;15(12):3254-3262. doi: 10.1111/os.13895. Epub 2023 Sep 27. Orthop Surg. 2023. PMID: 37753546 Free PMC article.
Cited by
-
Incidence and Risk Factors of Postoperative Delirium in Elderly Patients Following Hip Fracture Surgery: A Nationwide Retrospective Cohort Study in Taiwan.Int J Geriatr Psychiatry. 2025 May;40(5):e70094. doi: 10.1002/gps.70094. Int J Geriatr Psychiatry. 2025. PMID: 40354105 Free PMC article.
-
Effect of transcranial direct current stimulation on postoperative delirium in elderly patients undergoing hip fracture surgery: study protocol for a randomized controlled trial.Front Med (Lausanne). 2025 May 15;12:1558376. doi: 10.3389/fmed.2025.1558376. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40443512 Free PMC article.
References
-
- Loggers SAI, Van Lieshout EMM, Joosse P, Verhofstad MHJ, Willems HC. Prognosis of nonoperative treatment in elderly patients with a hip fracture: a systematic review and meta-analysis. Injury. 2020;51:2407–13. - PubMed
-
- Jay RH, Hipps D. Hip fracture-great steps forward but we still need better evidence. A commentary on NICE CG124 and QS16 on fractured neck of femur. Age Ageing. 2018;47:630–2. - PubMed
-
- Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018;49:1458–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
