

Bile acid profiles and classification model accuracy for inflammatory bowel disease diagnosis
- PMID: 38847684
- PMCID: PMC11155534
- DOI: 10.1097/MD.0000000000038457
Bile acid profiles and classification model accuracy for inflammatory bowel disease diagnosis
Abstract
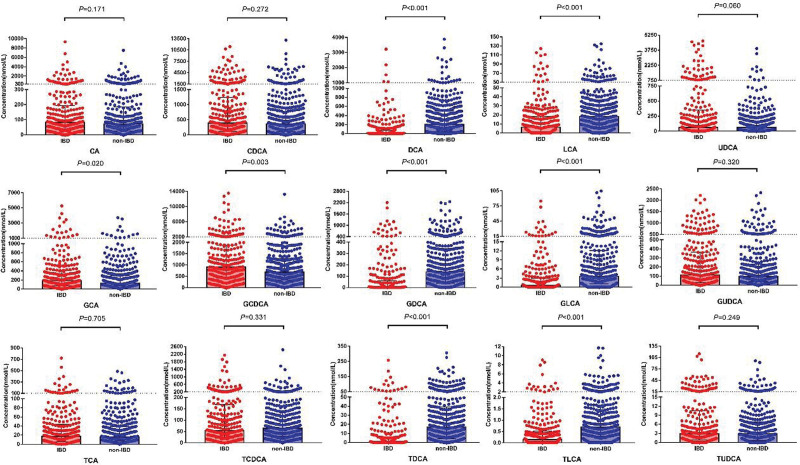
To investigate the utility of serum bile acid profiling for the diagnosis of inflammatory bowel disease (IBD). We analyzed 15 specific bile acids in the serum of 269 IBD patients, 200 healthy controls (HC), and 174 patients with other intestinal diseases (OID) using liquid chromatography-tandem mass spectrometry (LC-MS/MS). Serum bile acid levels were compared between IBD group, HC group, and OID group. Binary logistic regression-based models were developed to model the bile acids and diagnose IBD. Furthermore, receiver operating characteristic (ROC) curve analysis was performed to assess the diagnostic accuracy of each bile acid and the model. Compared to HC group, IBD group exhibited significantly lower levels of chenodeoxycholic acid (CDCA), deoxycholic acid (DCA), glycodeoxycholic acid (GDCA), taurodeoxycholic acid (TDCA), lithocholic acid (LCA), glycolithocholic acid (GLCA), taurolithocholic acid (TLCA), and an elevated primary-to-secondary bile acid ratio. DCA had an area under the curve (AUC) of 0.860 for diagnosing IBD, with a sensitivity of 80.67% and a specificity of 82.50%. A model Y0 combining DCA and CDCA to distinguish between IBD group and HC group further improved accuracy (AUC = 0.866, sensitivity = 76.28%, specificity = 89.37%). Compared to non-IBD group (which combined healthy controls and those with other intestinal diseases), IBD group had significantly lower levels of DCA, GDCA, TDCA, LCA, GLCA, and TLCA, and elevated levels of glycocholic acid (GCA) and glycochenodeoxycholic acid (GCDCA). A model Y1 incorporating GCDCA, DCA and TLCA to distinguish between IBD group and non-IBD group yielded an AUC of 0.792, with a sensitivity of 77.67% and specificity of 71.91%. IBD patients exhibit decreased serum secondary bile acid levels and an elevated primary-to-secondary bile acid ratio. Serum bile acid alterations are associated with the onset of IBD. A model consisting of CDCA and DCA has potential for distinguishing between IBD group and HC group, while a model incorporating GCDCA, DCA and TLCA may be suitable for distinguishing between IBD group and non-IBD group.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Torres J, Mehandru S, Colombel JF, et al. . Crohn’s disease. Lancet (London, England). 2017;389:1741–55. - PubMed
-
- Ng SC, Shi HY, Hamidi N, et al. . Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet (London, England). 2017;390:2769–78. - PubMed
-
- Kaplan GG, Ng SC. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterology. 2017;152:313–21.e2. - PubMed
-
- Gomollón F, Dignass A, Annese V, et al. . 3rd European evidence-based consensus on the diagnosis and management of Crohn’s Disease 2016: Part 1: diagnosis and medical management. J Crohns Colitis. 2017;11:3–25. - PubMed
-
- Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018, Beijing). J Dig Dis. 2021;22:298–317. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
