

Prediction of gait recovery using machine learning algorithms in patients with spinal cord injury
- PMID: 38847729
- PMCID: PMC11155515
- DOI: 10.1097/MD.0000000000038286
Prediction of gait recovery using machine learning algorithms in patients with spinal cord injury
Abstract
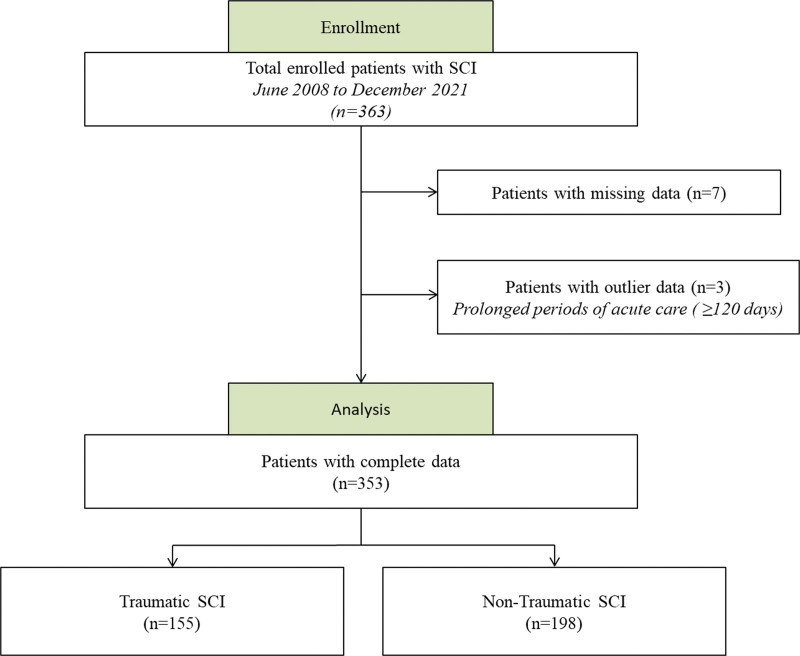
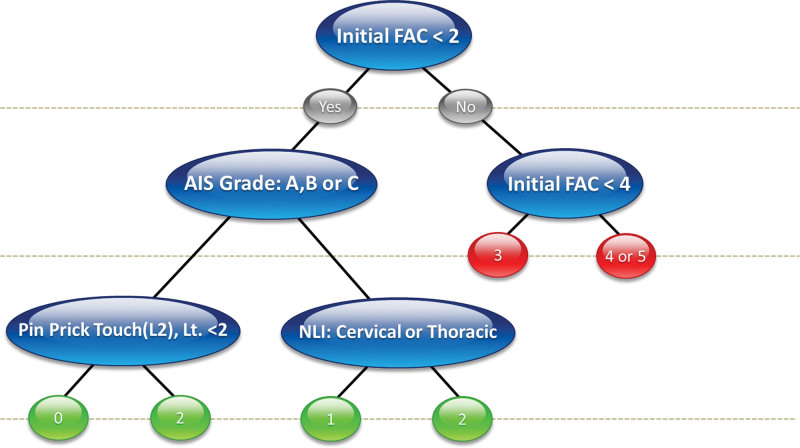
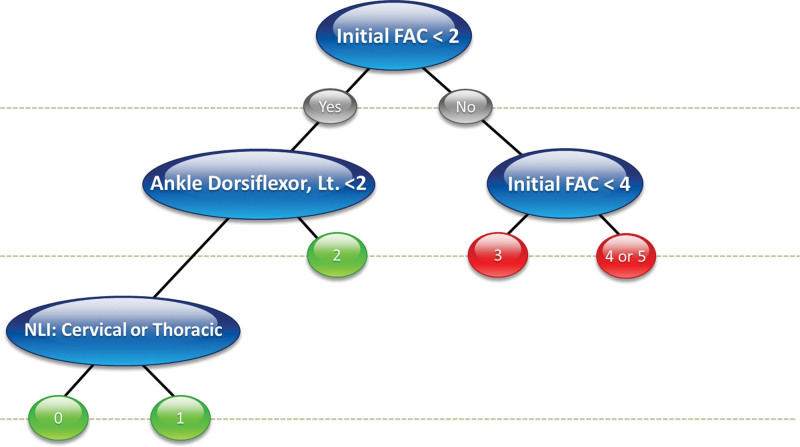
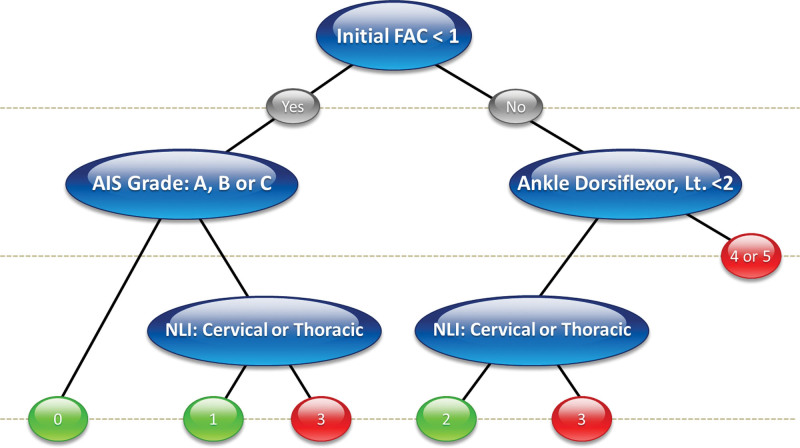
With advances in artificial intelligence, machine learning (ML) has been widely applied to predict functional outcomes in clinical medicine. However, there has been no attempt to predict walking ability after spinal cord injury (SCI) based on ML. In this situation, the main purpose of this study was to predict gait recovery after SCI at discharge from an acute rehabilitation facility using various ML algorithms. In addition, we explored important variables that were related to the prognosis. Finally, we attempted to suggest an ML-based decision support system (DSS) for predicting gait recovery after SCI. Data were collected retrospectively from patients with SCI admitted to an acute rehabilitation facility between June 2008 to December 2021. Linear regression analysis and ML algorithms (random forest [RF], decision tree [DT], and support vector machine) were used to predict the functional ambulation category at the time of discharge (FAC_DC) in patients with traumatic or non-traumatic SCI (n = 353). The independent variables were age, sex, duration of acute care and rehabilitation, comorbidities, neurological information entered into the International Standards for Neurological Classification of SCI worksheet, and somatosensory-evoked potentials at the time of admission to the acute rehabilitation facility. In addition, the importance of variables and DT-based DSS for FAC_DC was analyzed. As a result, RF and DT accurately predicted the FAC_DC measured by the root mean squared error. The root mean squared error of RF and the DT were 1.09 and 1.24 for all participants, 1.20 and 1.06 for those with trauma, and 1.12 and 1.03 for those with non-trauma, respectively. In the analysis of important variables, the initial FAC was found to be the most influential factor in all groups. In addition, we could provide a simple DSS based on strong predictors such as the initial FAC, American Spinal Injury Association Impairment Scale grades, and neurological level of injury. In conclusion, we provide that ML can accurately predict gait recovery after SCI for the first time. By focusing on important variables and DSS, we can guide early prognosis and establish personalized rehabilitation strategies in acute rehabilitation hospitals.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D. A global map for traumatic spinal cord injury epidemiology: towards a living data repository for injury prevention. Spinal Cord. 2011;49:493–501. - PubMed
-
- New PW, Cripps RA, Bonne Lee B. Global maps of non-traumatic spinal cord injury epidemiology: towards a living data repository. Spinal Cord. 2014;52:97–109. - PubMed
-
- Kirshblum SC, Priebe MM, Ho CH, Scelza WM, Chiodo AE, Wuermser LA. Spinal cord injury medicine. 3. Rehabilitation phase after acute spinal cord injury. Arch Phys Med Rehabil. 2007;88(3 Suppl 1):S62–70. - PubMed
-
- Burns AS, Ditunno JF. Establishing prognosis and maximizing functional outcomes after spinal cord injury: a review of current and future directions in rehabilitation management. Spine (Phila Pa 1976). 2001;26(24 Suppl):S137–45. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
