

Polygenic risk score adds to a clinical risk score in the prediction of cardiovascular disease in a clinical setting
- PMID: 38848106
- PMCID: PMC11379490
- DOI: 10.1093/eurheartj/ehae342
Polygenic risk score adds to a clinical risk score in the prediction of cardiovascular disease in a clinical setting
Abstract
Background and aims: A cardiovascular disease polygenic risk score (CVD-PRS) can stratify individuals into different categories of cardiovascular risk, but whether the addition of a CVD-PRS to clinical risk scores improves the identification of individuals at increased risk in a real-world clinical setting is unknown.
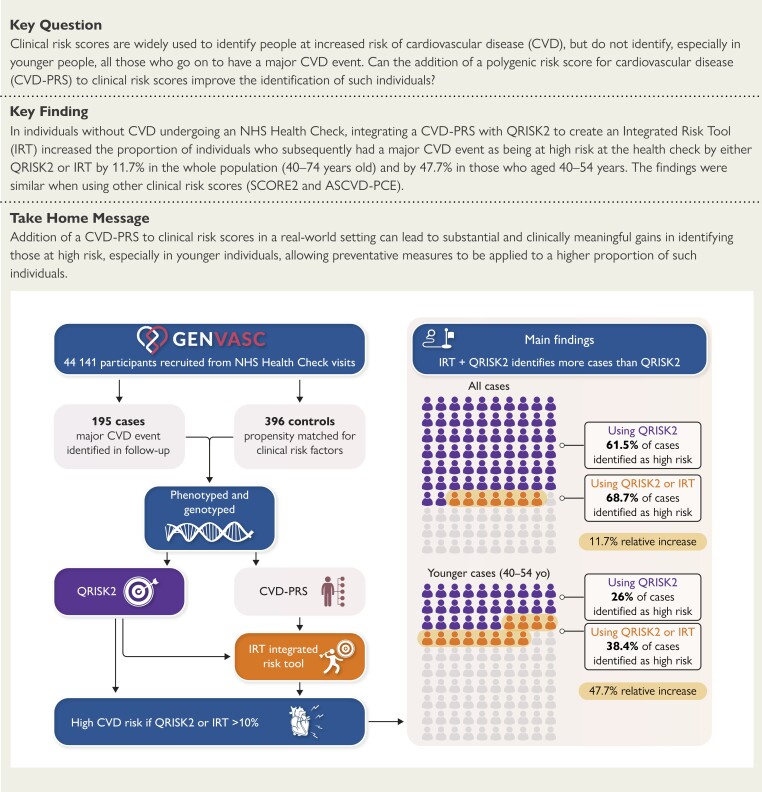
Methods: The Genetics and the Vascular Health Check Study (GENVASC) was embedded within the UK National Health Service Health Check (NHSHC) programme which invites individuals between 40-74 years of age without known CVD to attend an assessment in a UK general practice where CVD risk factors are measured and a CVD risk score (QRISK2) is calculated. Between 2012-2020, 44,141 individuals (55.7% females, 15.8% non-white) who attended an NHSHC in 147 participating practices across two counties in England were recruited and followed. When 195 individuals (cases) had suffered a major CVD event (CVD death, myocardial infarction or acute coronary syndrome, coronary revascularisation, stroke), 396 propensity-matched controls with a similar risk profile were identified, and a nested case-control genetic study undertaken to see if the addition of a CVD-PRS to QRISK2 in the form of an integrated risk tool (IRT) combined with QRISK2 would have identified more individuals at the time of their NHSHC as at high risk (QRISK2 10-year CVD risk of ≥10%), compared with QRISK2 alone.
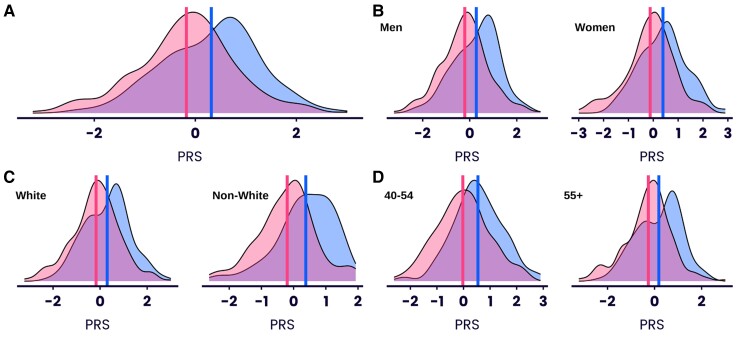
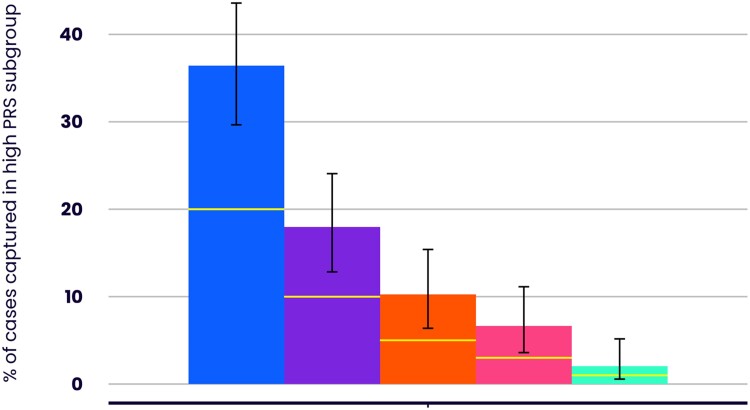
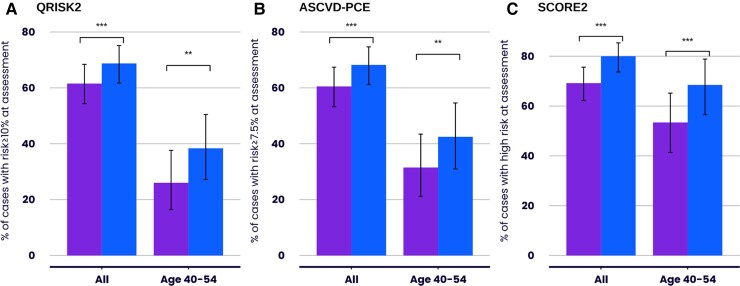
Results: The distribution of the standardised CVD-PRS was significantly different in cases compared with controls (cases mean score .32; controls, -.18, P = 8.28×10-9). QRISK2 identified 61.5% (95% confidence interval [CI]: 54.3%-68.4%) of individuals who subsequently developed a major CVD event as being at high risk at their NHSHC, while the combination of QRISK2 and IRT identified 68.7% (95% CI: 61.7%-75.2%), a relative increase of 11.7% (P = 1×10-4). The odds ratio (OR) of being up-classified was 2.41 (95% CI: 1.03-5.64, P = .031) for cases compared with controls. In individuals aged 40-54 years, QRISK2 identified 26.0% (95% CI: 16.5%-37.6%) of those who developed a major CVD event, while the combination of QRISK2 and IRT identified 38.4% (95% CI: 27.2%-50.5%), indicating a stronger relative increase of 47.7% in the younger age group (P = .001). The combination of QRISK2 and IRT increased the proportion of additional cases identified similarly in women as in men, and in non-white ethnicities compared with white ethnicity. The findings were similar when the CVD-PRS was added to the atherosclerotic cardiovascular disease pooled cohort equations (ASCVD-PCE) or SCORE2 clinical scores.
Conclusions: In a clinical setting, the addition of genetic information to clinical risk assessment significantly improved the identification of individuals who went on to have a major CVD event as being at high risk, especially among younger individuals. The findings provide important real-world evidence of the potential value of implementing a CVD-PRS into health systems.
Keywords: ASCVD-PCE; CVD risk assessment; Polygenic risk scores; QRISK2; SCORE2.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Iribarren C, Lu M, Jorgenson E, Martínez M, Lluis-Ganella C, Subirana I, et al. . Clinical utility of multimarker genetic risk scores for prediction of incident coronary heart disease: a cohort study among over 51 000 individuals of European ancestry. Circ Cardiovasc Genet 2016;9:531–40. 10.1161/CIRCGENETICS.116.001522 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
