

Alcoholic cardiomyopathy: an update
- PMID: 38848133
- PMCID: PMC11231944
- DOI: 10.1093/eurheartj/ehae362
Alcoholic cardiomyopathy: an update
Abstract
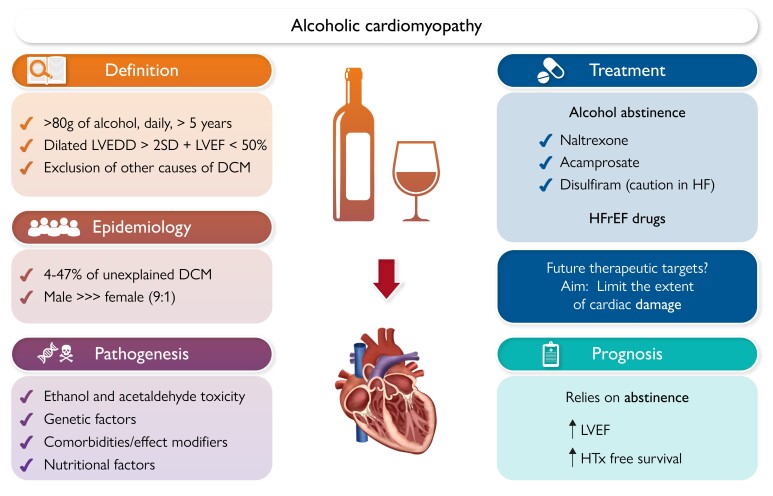
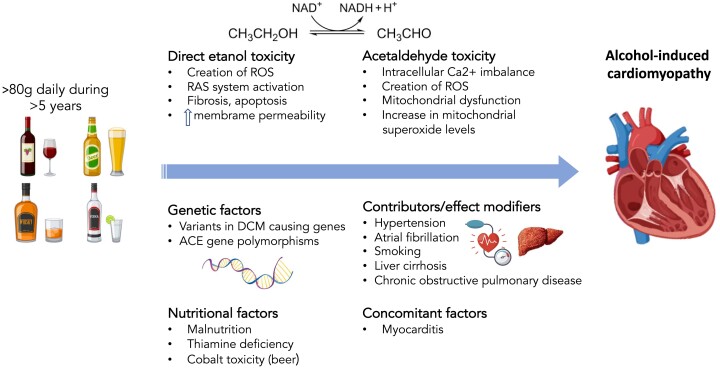
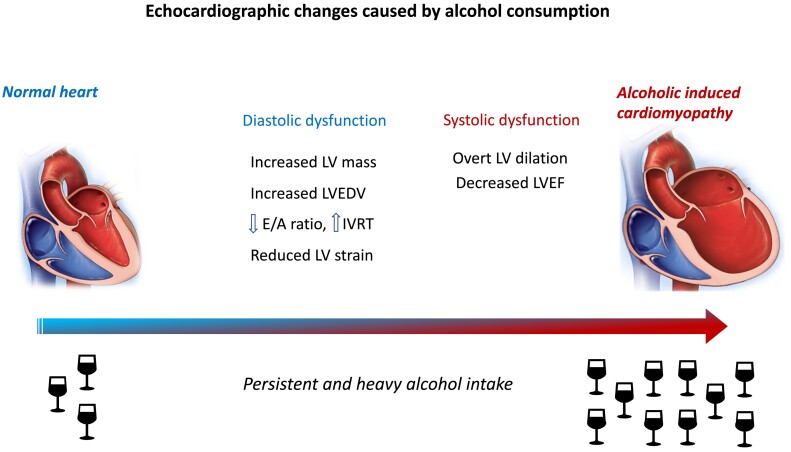
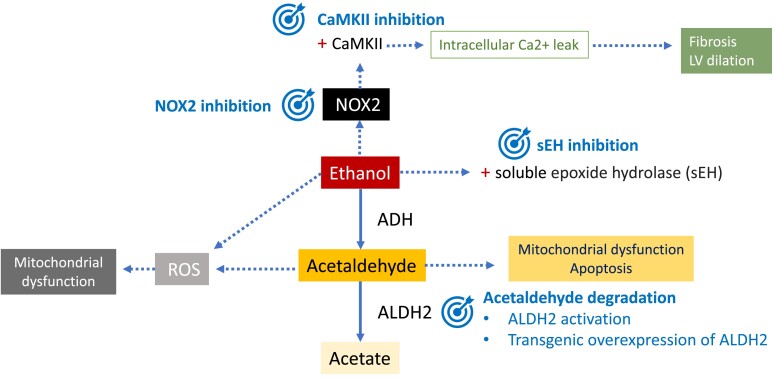
Alcohol-induced cardiomyopathy (AC) is an acquired form of dilated cardiomyopathy (DCM) caused by prolonged and heavy alcohol intake in the absence of other causes. The amount of alcohol required to produce AC is generally considered as >80 g/day over 5 years, but there is still some controversy regarding this definition. This review on AC focuses on pathogenesis, which involves different mechanisms. Firstly, the direct toxic effect of ethanol promotes oxidative stress in the myocardium and activation of the renin-angiotensin system. Moreover, acetaldehyde, the best-studied metabolite of alcohol, can contribute to myocardial damage impairing actin-myosin interaction and producing mitochondrial dysfunction. Genetic factors are also involved in the pathogenesis of AC, with DCM-causing genetic variants in patients with AC, especially titin-truncating variants. These findings support a double-hit hypothesis in AC, combining genetics and environmental factors. The synergistic effect of alcohol with concomitant conditions such as hypertension or liver cirrhosis can be another contributing factor leading to AC. There are no specific cardiac signs and symptoms in AC as compared with other forms of DCM. However, natural history of AC differs from DCM and relies directly on alcohol withdrawal, as left ventricular ejection fraction recovery in abstainers is associated with an excellent prognosis. Thus, abstinence from alcohol is the most crucial step in treating AC, and specific therapies are available for this purpose. Otherwise, AC should be treated according to current guidelines of heart failure with reduced ejection fraction. Targeted therapies based on AC pathogenesis are currently being developed and could potentially improve AC treatment in the future.
Keywords: Alcohol; Alcoholic cardiomyopathy; Pathogenesis; Treatment.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Poznyak V, Reve D. Global status report on alcohol and health 2018 n.d. https://www.who.int/publications/i/item/9789241565639. Date accessed 9 June 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
