

Beyond the visible: preliminary evaluation of the first wearable augmented reality assistance system for pancreatic surgery
- PMID: 38849631
- PMCID: PMC11757645
- DOI: 10.1007/s11548-024-03131-0
Beyond the visible: preliminary evaluation of the first wearable augmented reality assistance system for pancreatic surgery
Abstract
Purpose: The retroperitoneal nature of the pancreas, marked by minimal intraoperative organ shifts and deformations, makes augmented reality (AR)-based systems highly promising for pancreatic surgery. This study presents preliminary data from a prospective study aiming to develop the first wearable AR assistance system, ARAS, for pancreatic surgery and evaluating its usability, accuracy, and effectiveness in enhancing the perioperative outcomes of patients.
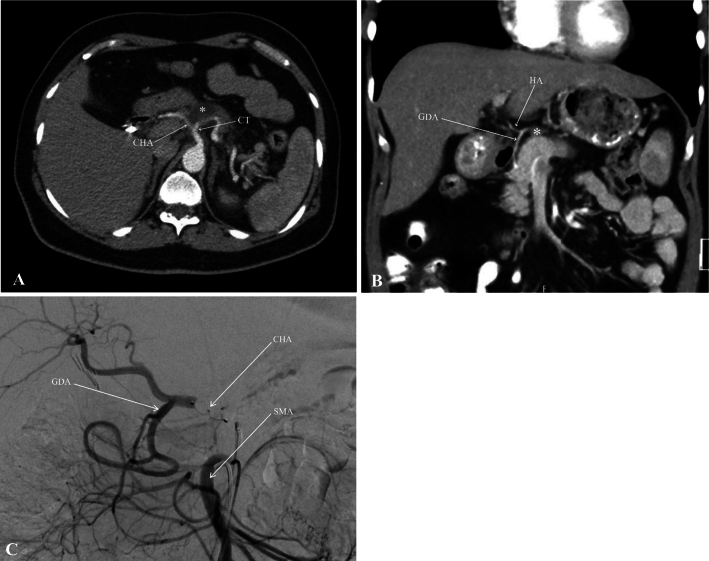
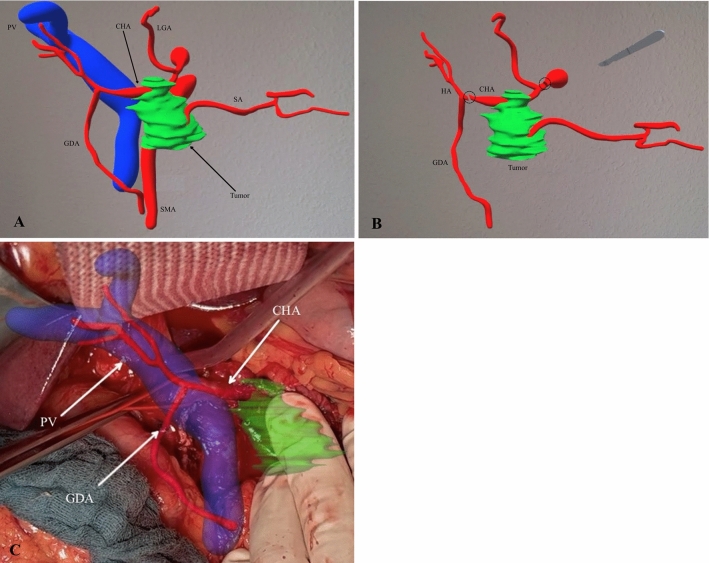
Methods: We developed ARAS as a two-phase system for a wearable AR device to aid surgeons in planning and operation. This system was used to visualize and register patient-specific 3D anatomical models during the surgery. The location and precision of the registered 3D anatomy were evaluated by assessing the arterial pulse and employing Doppler and duplex ultrasonography. The usability, accuracy, and effectiveness of ARAS were assessed using a five-point Likert scale questionnaire.
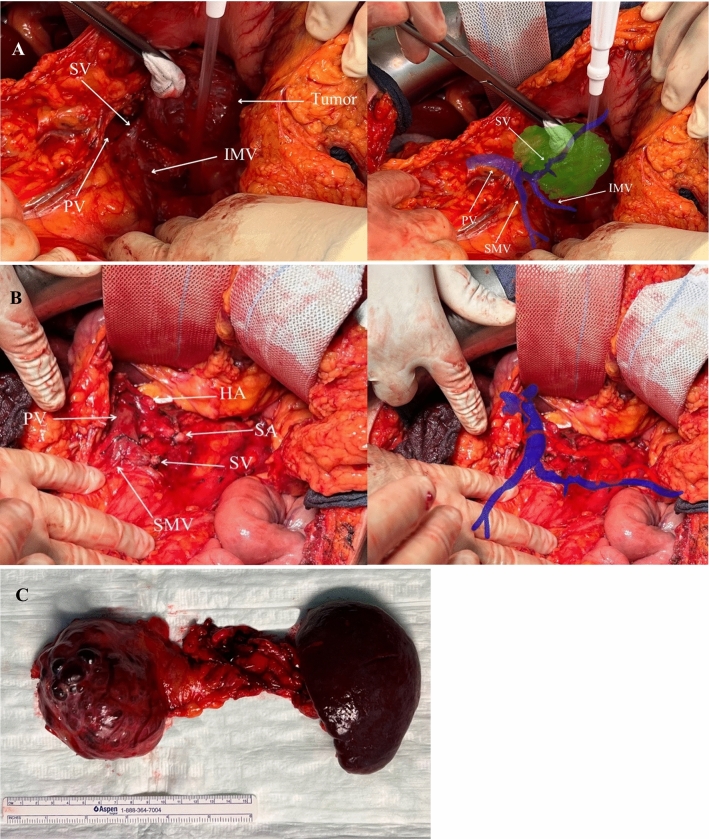
Results: Perioperative outcomes of five patients underwent various pancreatic resections with ARAS are presented. Surgeons rated ARAS as excellent for preoperative planning. All structures were accurately identified without any noteworthy errors. Only tumor identification decreased after the preparation phase, especially in patients who underwent pancreaticoduodenectomy because of the extensive mobilization of peripancreatic structures. No perioperative complications related to ARAS were observed.
Conclusions: ARAS shows promise in enhancing surgical precision during pancreatic procedures. Its efficacy in preoperative planning and intraoperative vascular identification positions it as a valuable tool for pancreatic surgery and a potential educational resource for future surgical residents.
Keywords: Augmented reality; Navigation system; Pancreatectomy; Surgical planning; Wearable devices.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no competing interests to declare that are relevant to the content of this article. Ethical approval: The study protocol was approved by the Ethics Committee of the Medical Association of Saarland (registration number: 159/23).
Figures



References
-
- Siegel RL, Miller KD, Jemal A (2018) Cancer statistics, 2018. CA Cancer J Clin 68:7–30 - PubMed
-
- Heestand GM, Murphy JD, Lowy AM (2015) Approach to patients with pancreatic cancer without detectable metastases. J Clin Oncol 33:1770–1778 - PubMed
-
- Braga M, Capretti G, Pecorelli N, Balzano G, Doglioni C, Ariotti R, Di Carlo V (2011) A prognostic score to predict major complications after pancreaticoduodenectomy. Ann Surg 254:702–708 - PubMed
-
- Sánchez-Velázquez P, Muller X, Malleo G, Park J-S, Hwang H-K, Napoli N, Javed AA, Inoue Y, Beghdadi N, Kalisvaart M (2019) Benchmarks in pancreatic surgery: a novel tool for unbiased outcome comparisons. Ann Surg 270:211–218 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
