

Opening the doors of precision medicine: novel tools to assess intestinal barrier in inflammatory bowel disease and colitis-associated neoplasia
- PMID: 38851294
- PMCID: PMC11422792
- DOI: 10.1136/gutjnl-2023-331579
Opening the doors of precision medicine: novel tools to assess intestinal barrier in inflammatory bowel disease and colitis-associated neoplasia
Abstract
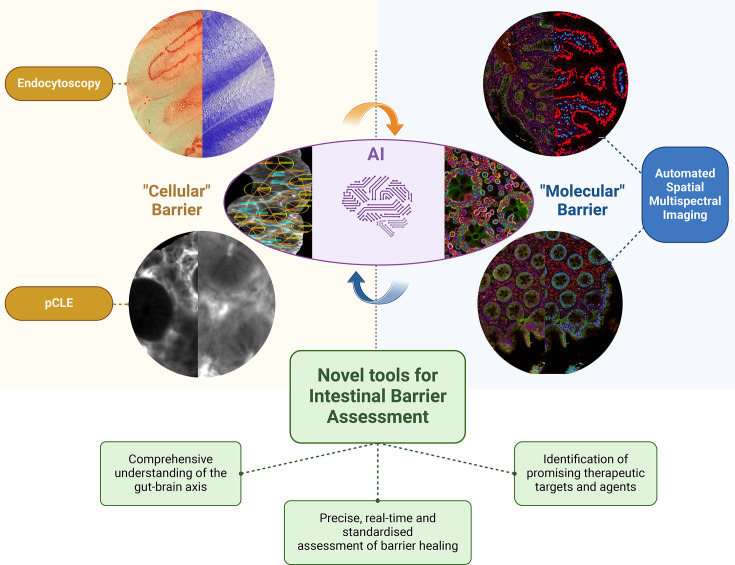
Mounting evidence underscores the pivotal role of the intestinal barrier and its convoluted network with diet and intestinal microbiome in the pathogenesis of inflammatory bowel disease (IBD) and colitis-associated colorectal cancer (CRC). Moreover, the bidirectional association of the intestinal barrier with the liver and brain, known as the gut-brain axis, plays a crucial role in developing complications, including extraintestinal manifestations of IBD and CRC metastasis. Consequently, barrier healing represents a crucial therapeutic target in these inflammatory-dependent disorders, with barrier assessment predicting disease outcomes, response to therapy and extraintestinal manifestations.New advanced technologies are revolutionising our understanding of the barrier paradigm, enabling the accurate assessment of the intestinal barrier and aiding in unravelling the complexity of the gut-brain axis. Cutting-edge endoscopic imaging techniques, such as ultra-high magnification endocytoscopy and probe-based confocal laser endomicroscopy, are new technologies allowing real-time exploration of the 'cellular' intestinal barrier. Additionally, novel advanced spatial imaging technology platforms, including multispectral imaging, upconversion nanoparticles, digital spatial profiling, optical spectroscopy and mass cytometry, enable a deep and comprehensive assessment of the 'molecular' and 'ultrastructural' barrier. In this promising landscape, artificial intelligence plays a pivotal role in standardising and integrating these novel tools, thereby contributing to barrier assessment and prediction of outcomes.Looking ahead, this integrated and comprehensive approach holds the promise of uncovering new therapeutic targets, breaking the therapeutic ceiling in IBD. Novel molecules, dietary interventions and microbiome modulation strategies aim to restore, reinforce, or modulate the gut-brain axis. These advancements have the potential for transformative and personalised approaches to managing IBD.
Keywords: BRAIN/GUT INTERACTION; ENDOSCOPY; GASTROINTESTINAL CANCER; INFLAMMATORY BOWEL DISEASE; INTESTINAL BARRIER FUNCTION.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Ananthakrishnan AN, Kaplan GG, Bernstein CN, et al. Lifestyle, behaviour, and environmental modification for the management of patients with inflammatory bowel diseases: an international organization for study of inflammatory bowel diseases consensus. Lancet Gastroenterol Hepatol. 2022;7:666–78. doi: 10.1016/S2468-1253(22)00021-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources