

Historical neighborhood redlining and bystander CPR disparities in out-of-hospital cardiac arrest
- PMID: 38851447
- PMCID: PMC12046434
- DOI: 10.1016/j.resuscitation.2024.110264
Historical neighborhood redlining and bystander CPR disparities in out-of-hospital cardiac arrest
Abstract
Background: Out-of-hospital cardiac arrest (OHCA) is associated with low survival rates. Bystander cardiopulmonary resuscitation (CPR) is essential for improving outcomes, but its utilization remains limited, particularly among racial and ethnic minorities. Historical redlining, a practice that classified neighborhoods for mortgage risk in 1930s, may have lasting implications for social and health outcomes. This study sought to investigate the influence of redlining on the provision of bystander CPR during witnessed OHCA.
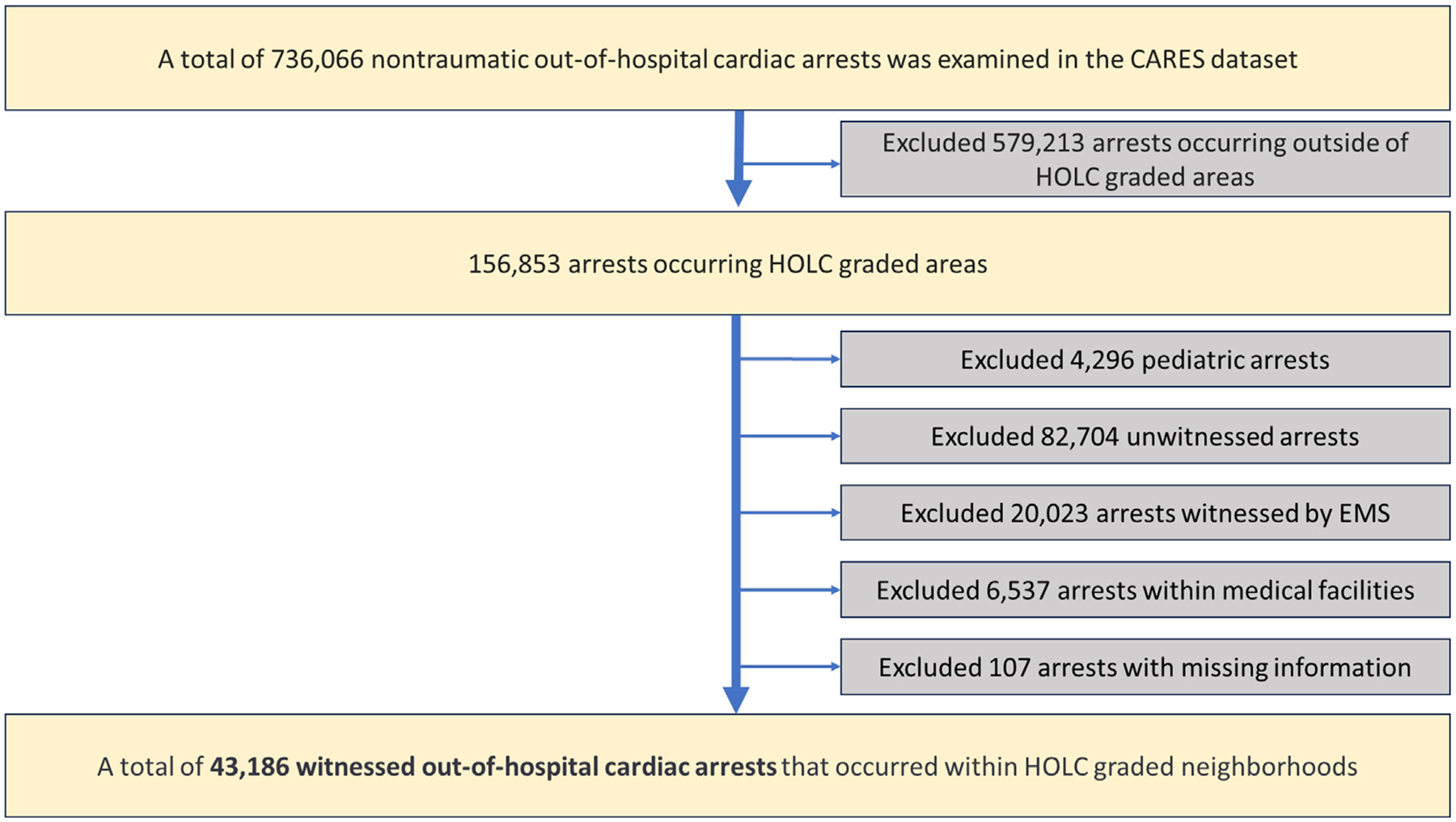
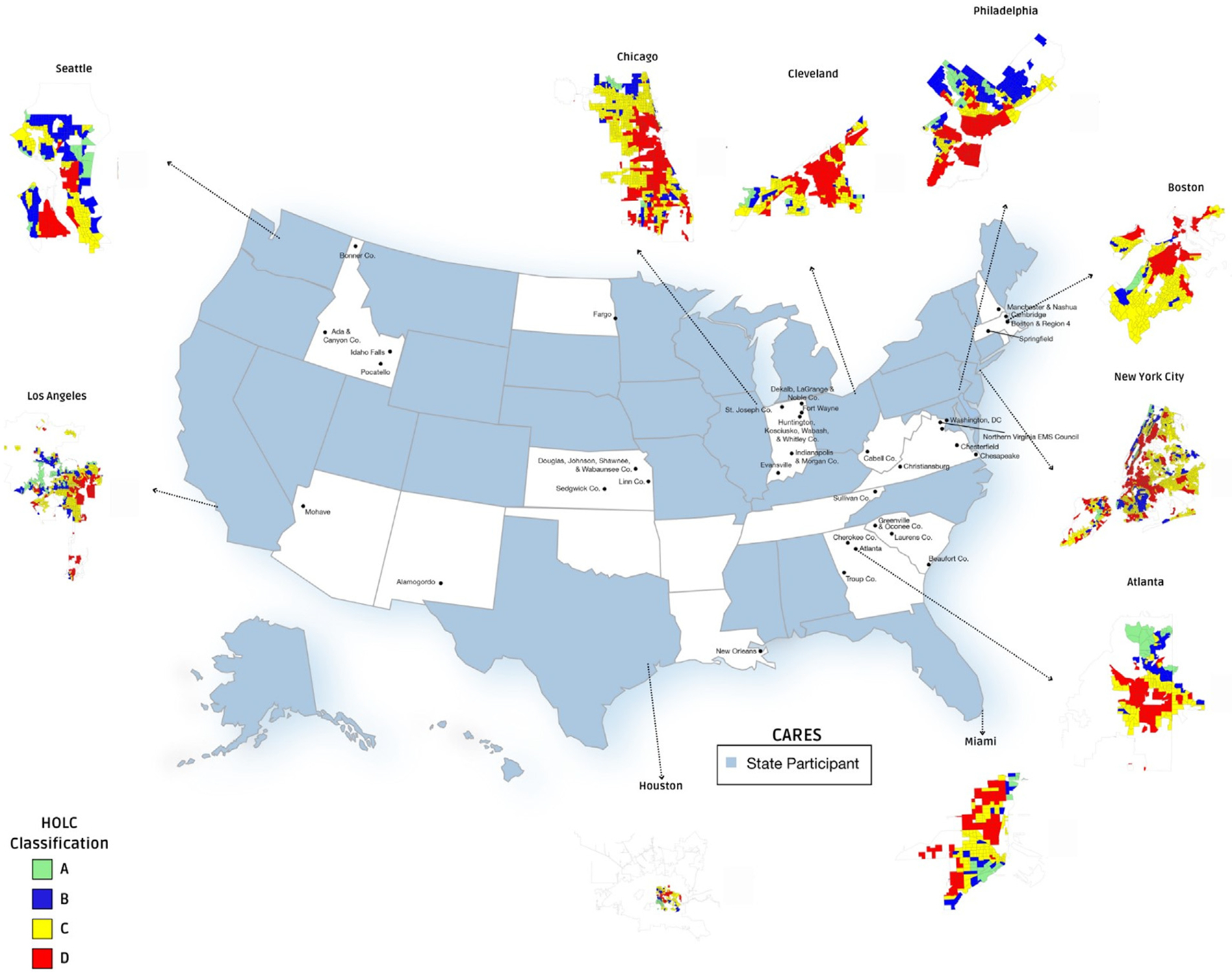
Methods: We conducted an analysis using data from the comprehensive Cardiac Arrest Registry to Enhance Survival (CARES), encompassing 736,066 non-traumatic OHCA cases across the United States. The Home Owners' Loan Corporation (HOLC) map shapefiles were utilized to categorize census tracts of arrests into four grades (A signifying "best", B "still desirable", C "declining", and D "hazardous"). Multivariable hierarchical logistic regression models were employed to predict the likelihood of CPR provision, adjusting for various factors including age, sex, race/ethnicity, arrest location, calendar year, and state of occurrence. Additionally, we accounted for the percentage of Black residents and residents below poverty levels at the census tract level.
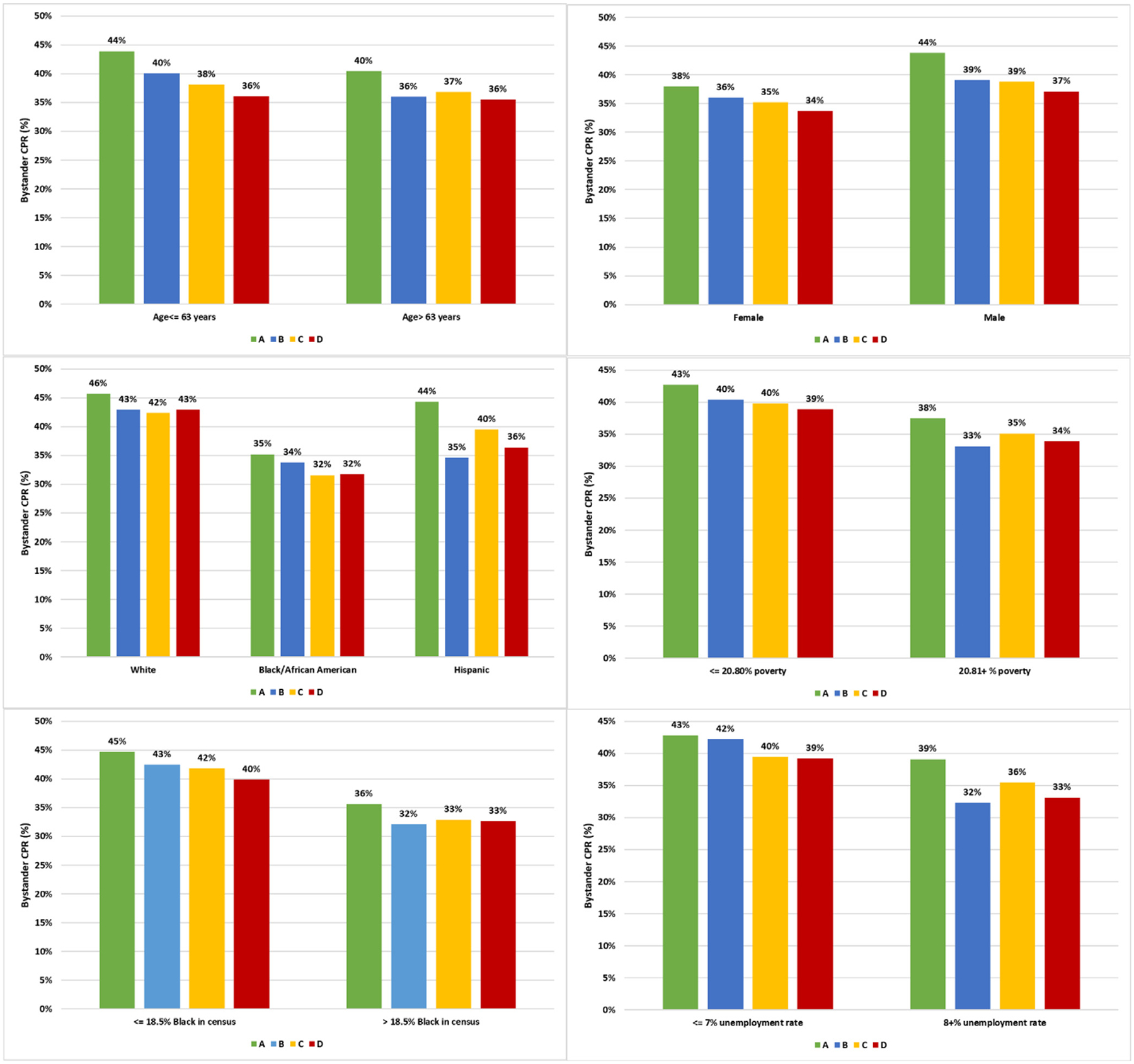
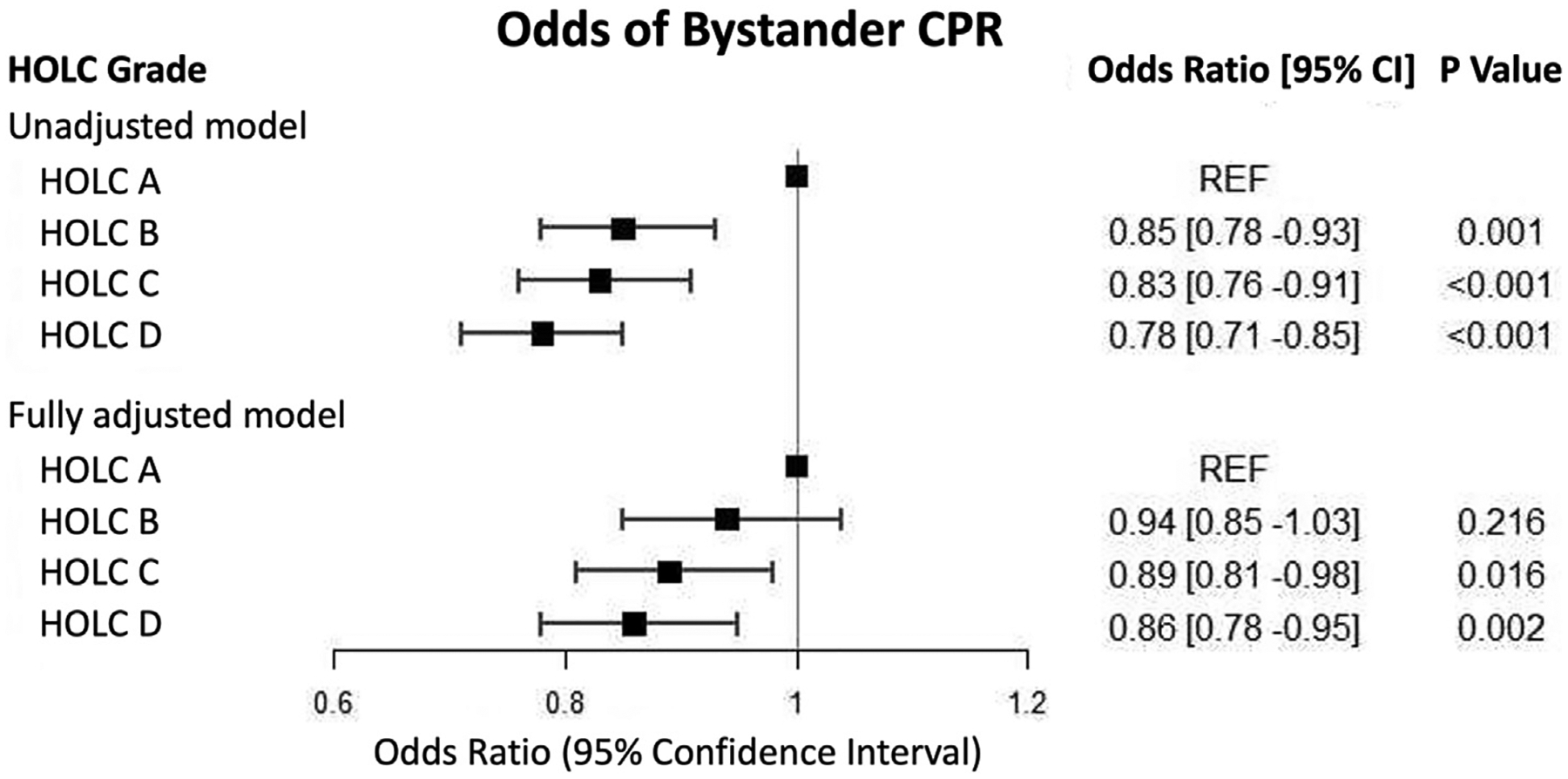
Results: Among the 43,186 witnessed cases of OHCA in graded HOLC census tracts, 37.2% received bystander CPR. The rates of bystander CPR exhibited a gradual decline across HOLC grades, ranging from 41.8% in HOLC grade A to 35.8% in HOLC grade D. In fully adjusted model, we observed significantly lower odds of receiving bystander CPR in HOLC grades C (OR 0.89, 95% CI 0.81-0.98, p = 0.016) and D (OR 0.86, 95% CI 0.78-0.95, p = 0.002) compared to HOLC grade A.
Conclusion: Redlining, a historical segregation practice, is associated with reduced contemporary rates of bystander CPR during OHCA. Targeted CPR training in redlined neighborhoods may be imperative to enhance survival outcomes.
Keywords: Bystander Cardiopulmonary Resuscitation; Cardiac Arrest Registry to Enhance Survival; Out-of-hospital cardiac arrest; Racial Disparities.
Copyright © 2024 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
