

Exoskeleton rehabilitation robot training for balance and lower limb function in sub-acute stroke patients: a pilot, randomized controlled trial
- PMID: 38851703
- PMCID: PMC11162020
- DOI: 10.1186/s12984-024-01391-0
Exoskeleton rehabilitation robot training for balance and lower limb function in sub-acute stroke patients: a pilot, randomized controlled trial
Abstract
Purpose: This pilot study aimed to investigate the effects of REX exoskeleton rehabilitation robot training on the balance and lower limb function in patients with sub-acute stroke.
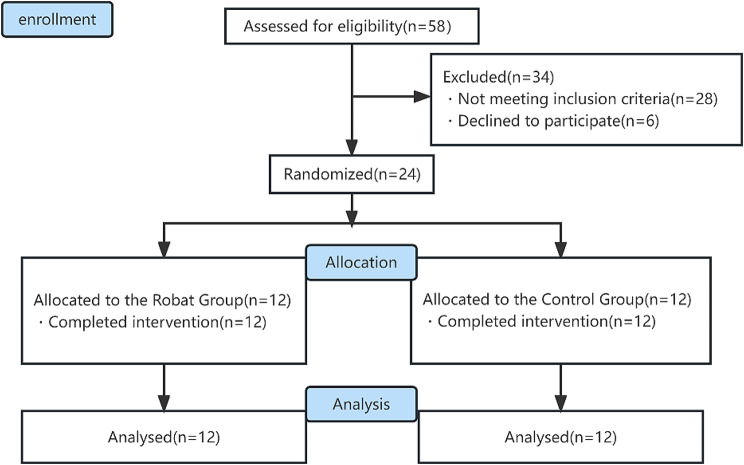
Methods: This was a pilot, single-blind, randomized controlled trial. Twenty-four patients with sub-acute stroke (with the course of disease ranging from 3 weeks to 3 months) were randomized into two groups, including a robot group and a control group. Patients in control group received upright bed rehabilitation (n = 12) and those in robot group received exoskeleton rehabilitation robot training (n = 12). The frequency of training in both groups was once a day (60 min each) for 5 days a week for a total of 4 weeks. Besides, the two groups were evaluated before, 2 weeks after and 4 weeks after the intervention, respectively. The primary assessment index was the Berg Balance Scale (BBS), whereas the secondary assessment indexes included the Fugl-Meyer Lower Extremity Motor Function Scale (FMA-LE), the Posture Assessment Scale for Stroke Patients (PASS), the Activities of Daily Living Scale (Modified Barthel Index, MBI), the Tecnobody Balance Tester, and lower extremity muscle surface electromyography (sEMG).
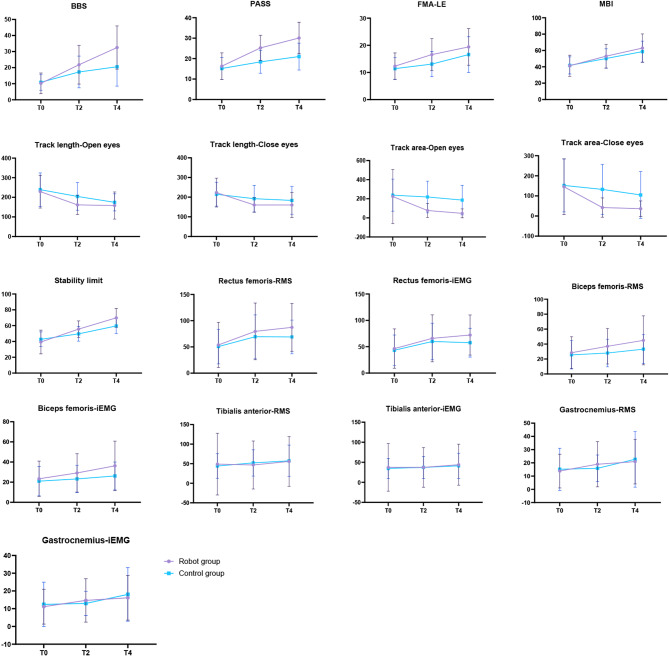
Results: The robot group showed significant improvements (P < 0.05) in the primary efficacy index BBS, as well as the secondary efficacy indexes PASS, FMA-LE, MBI, Tecnobody Balance Tester, and sEMG of the lower limb muscles. Besides, there were a significant differences in BBS, PASS, static eye-opening area or dynamic stability limit evaluation indexes between the robotic and control groups (P < 0.05).
Conclusions: This is the first study to investigate the effectiveness of the REX exoskeleton rehabilitation robot in the rehabilitation of patients with stroke. According to our results, the REX exoskeleton rehabilitation robot demonstrated superior potential efficacy in promoting the early recovery of balance and motor functions in patients with sub-acute stroke. Future large-scale randomized controlled studies and follow-up assessments are needed to validate the current findings.
Clinical trials registration: URL: https://www.chictr.org.cn/index.html.Unique identifier: ChiCTR2300068398.
Keywords: Balance function; Lower limb function; Rehabilitation robot; Stroke.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
We declare that we have no financial and personal relationships with other people ororganizations that can inappropriately influence our work, there is no professional orother personal interest of any nature or kind in any product, service and/or companythat could be construed as influencing the position presented in, or the review of, the manuscript entitled.
Figures

References
-
- WANG Y-J, LI Z-X, GU H-Q, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association. China Stroke Statistics: an update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations [J]. Stroke Vasc Neurol, 2022, 7(5): 415 – 50. - PMC - PubMed
-
- SHUMWAY-COOK A, ANSON D. Postural sway biofeedback: its effect on reestablishing stance stability in hemiplegic patients [J] Arch Phys Med Rehabil. 1988;69(6):395–400. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- No. WXTTP2020008/Wuxi 'Taihu Talent Plan' medical and health high-level talents project
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
- Y20212008/Wuxi Municipal Bureau on Science and Technology
LinkOut - more resources
Full Text Sources
Medical
