

Automatic analysis of nuclear features reveals a non-tumoral predictor of tumor grade in bladder cancer
- PMID: 38851736
- PMCID: PMC11162100
- DOI: 10.1186/s13000-024-01501-5
Automatic analysis of nuclear features reveals a non-tumoral predictor of tumor grade in bladder cancer
Abstract
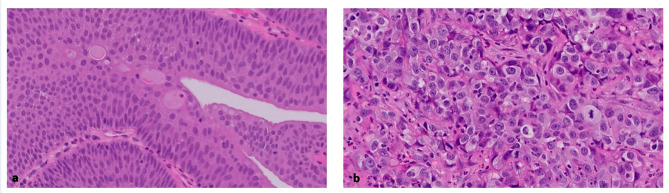
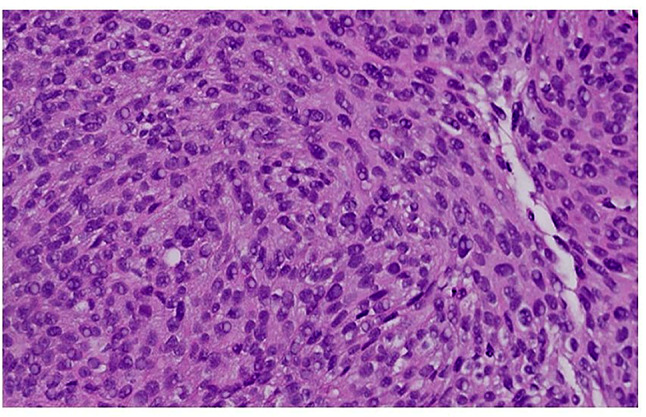
Background & objectives: Tumor grade determines prognosis in urothelial carcinoma. The classification of low and high grade is based on nuclear morphological features that include nuclear size, hyperchromasia and pleomorphism. These features are subjectively assessed by the pathologists and are not numerically measured, which leads to high rates of interobserver variability. The purpose of this study is to assess the value of a computer-based image analysis tool for identifying predictors of tumor grade in bladder cancer.
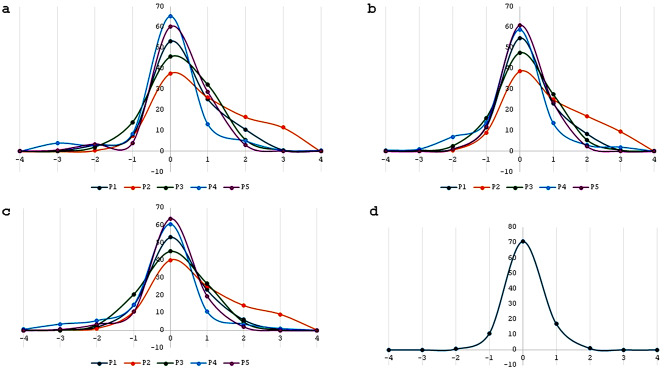
Methods: Four hundred images of urothelial tumors were graded by five pathologists and two expert genitourinary pathologists using a scale of 1 (lowest grade) to 5 (highest grade). A computer algorithm was used to automatically segment the nuclei and to provide morphometric parameters for each nucleus, which were used to establish the grading algorithm. Grading algorithm was compared to pathologists' agreement.
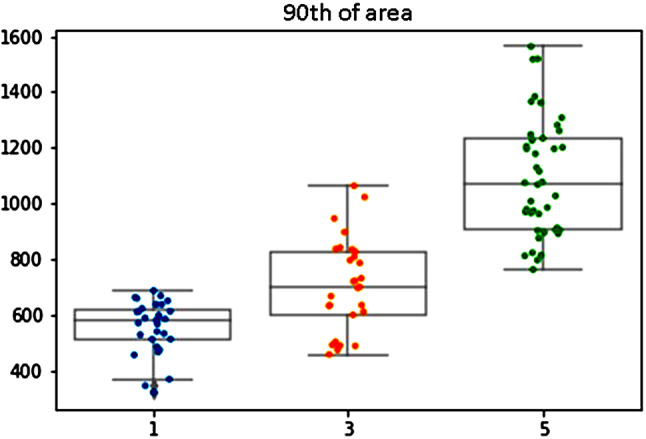
Results: Comparison of the grading scores of the five pathologists with the expert genitourinary pathologists score showed agreement rates between 88.5% and 97.5%.The agreement rate between the two expert genitourinary pathologists was 99.5%. The quantified algorithm based conventional parameters that determine the grade (nuclear size, pleomorphism and hyperchromasia) showed > 85% agreement with the expert genitourinary pathologists. Surprisingly, the parameter that was most associated with tumor grade was the 10th percentile of the nuclear area, and high grade was associated with lower 10th percentile nuclei, caused by the presence of more inflammatory cells in the high-grade tumors.
Conclusion: Quantitative nuclear features could be applied to determine urothelial carcinoma grade and explore new biologically explainable parameters with better correlation to grade than those currently used.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Sylvester RJ, Rodríguez O, Hernández V, et al. European Association of Urology (EAU) prognostic factor risk groups for non–muscle-invasive bladder Cancer (NMIBC) incorporating the WHO 2004/2016 and WHO 1973 classification systems for Grade: an update from the EAU NMIBC guidelines Panel[Formula present. Eur Urol. 2021;79(4):480–8. doi: 10.1016/j.eururo.2020.12.033. - DOI - PubMed
-
- Bol MG, Baak JP, Buhr-Wildhagen S, Kruse AJ, Kjellevold KH, Janssen EA, Mestad OØP. Reproducibility and prognostic variability of grade and lamina propria invasion in stages Ta, T1 urothelial carcinoma of the bladder. J Urol. 2003;169(4):1291–4. doi: 10.1097/01.ju.0000055471.78783.ae. - DOI - PubMed
-
- van der Kwast TH, Bubendorf L, Cheng L. International Society of Urological Pathology (ISUP) Consensus Conference on Current Issues in Bladder Cancer. American Journal of Surgical Pathology. 2024;48(1):1–3. 10.1097/PAS.0000000000002066. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
