

This is a preprint.
Association between Dietary Total Vitamin A, β-carotene, and Retinol Intake and Risk of cardiometabolic multimorbidity: Results from the China Health and Nutrition Survey, 1997-2015
- PMID: 38853914
- PMCID: PMC11160875
- DOI: 10.21203/rs.3.rs-4384704/v1
Association between Dietary Total Vitamin A, β-carotene, and Retinol Intake and Risk of cardiometabolic multimorbidity: Results from the China Health and Nutrition Survey, 1997-2015
Update in
-
Association between dietary vitamin A intake and risk of cardiometabolic multimorbidity.Sci Rep. 2024 Jul 19;14(1):16656. doi: 10.1038/s41598-024-67723-1. Sci Rep. 2024. PMID: 39030396 Free PMC article.
Abstract
Background: The association between vitamin A and single cardiometabolic diseases has been extensively studied, but the relationship between dietary vitamin A intake and the risk of cardiometabolic multimorbidity (CMM) has not been studied. Therefore, the present study was conducted to explore the association with CMM risk by analyzing different sources of vitamin A.
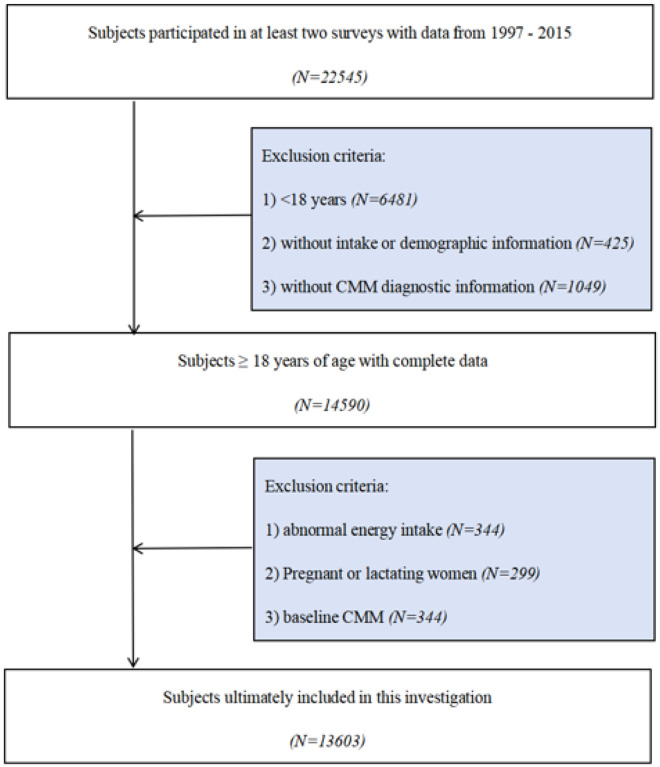
Methods: This study utilized 13,603 subjects aged ≥ 18 years from 1997-2015 from the China Health and Nutrition Survey (CHNS). Dietary intake was calculated from 3 consecutive 24-h dietary recalls combined with a house hold food inventory. CMM is defined as the development of at least two cardiometabolic diseases.
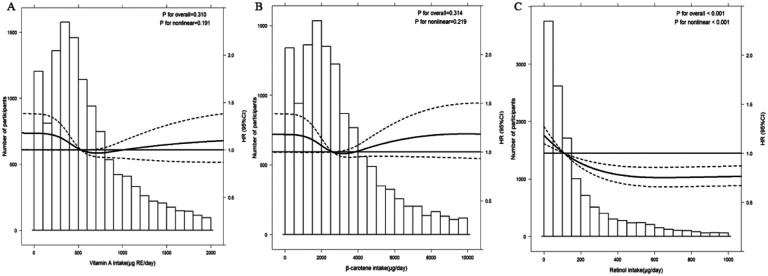
Results: After a median follow-up of 9.1 years, there were 1050 new cases of CMM. The risk of CMM was significantly lower in those with higher vitamin A intake (Q1 vs Q5 HR 0.66, 95% CI 0.54-0.81). β-carotene (Q1 vs Q5 HR 0.82, 95% CI 0.66-1.02) and retinol (Q1 vs Q5 HR 0.59, 95%CI 0.48-0.73) intake had a similarly negative correlation. Using restricted cubic spline found an L-shaped relationship between retinol intake and CMM (p non-linear < 0.001). In subgroup analyses, protective effects were stronger for participants aged ≥ 44 years (HR 0.72, 95%CI 0.57-0.92) and for the female group (HR 0.62, 95%CI 0.45-0.84).
Conclusion: Dietary vitamin A was a protective factor for CMM, and this effect was stronger in age ≥ 44 years and in the female group. There was a ceiling effect on the protective effect of retinol intake on the risk of CMM.
Keywords: Cardiometabolic multimorbidity; Prospective cohort study; retinol; vitamin A; β-carotene.
Conflict of interest statement
Declarations of interest: The authors have no relevant financial or non-financial interests to disclose.
Figures
Similar articles
-
Association between dietary vitamin A intake and risk of cardiometabolic multimorbidity.Sci Rep. 2024 Jul 19;14(1):16656. doi: 10.1038/s41598-024-67723-1. Sci Rep. 2024. PMID: 39030396 Free PMC article.
-
Dietary Total Vitamin A, β-carotene, and Retinol Intake and the Risk of Diabetes in Chinese Adults with Plant-based Diets.J Clin Endocrinol Metab. 2022 Sep 28;107(10):e4106-e4114. doi: 10.1210/clinem/dgac439. J Clin Endocrinol Metab. 2022. PMID: 35868629 Free PMC article.
-
Obesity, composite dietary antioxidant index, and their interactive association with the risk of cardiometabolic multimorbidity in the elderly from a large national survey.Lipids Health Dis. 2025 Apr 9;24(1):132. doi: 10.1186/s12944-025-02549-y. Lipids Health Dis. 2025. PMID: 40205470 Free PMC article.
-
Correlation of cardiometabolic index and sarcopenia with cardiometabolic multimorbidity in middle-aged and older adult: a prospective study.Front Endocrinol (Lausanne). 2024 May 28;15:1387374. doi: 10.3389/fendo.2024.1387374. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38863933 Free PMC article.
-
Serum/plasma biomarkers and the progression of cardiometabolic multimorbidity: a systematic review and meta-analysis.Front Public Health. 2023 Nov 23;11:1280185. doi: 10.3389/fpubh.2023.1280185. eCollection 2023. Front Public Health. 2023. PMID: 38074721 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
