

This is a preprint.
Impact of Cerebrospinal Fluid Leukocyte Infiltration and Neuroimmmune Mediators on Survival with HIV-Associated Cryptococcal Meningitis
- PMID: 38854002
- PMCID: PMC11160828
- DOI: 10.1101/2024.05.29.24308130
Impact of Cerebrospinal Fluid Leukocyte Infiltration and Neuroimmmune Mediators on Survival with HIV-Associated Cryptococcal Meningitis
Update in
-
Impact of cerebrospinal fluid leukocyte infiltration and activated neuroimmune mediators on survival with HIV-associated cryptococcal meningitis.PLoS Negl Trop Dis. 2025 Feb 10;19(2):e0012873. doi: 10.1371/journal.pntd.0012873. eCollection 2025 Feb. PLoS Negl Trop Dis. 2025. PMID: 39928682 Free PMC article.
Abstract
Introduction: Cryptococcal meningitis remains a prominent cause of death in persons with advanced HIV disease. CSF leukocyte infiltration predicts survival at 18 weeks; however, how CSF immune response relates to CSF leukocyte infiltration is unknown.
Methods: We enrolled 401 adults with HIV-associated cryptococcal meningitis in Uganda who received amphotericin and fluconazole induction therapy. We assessed the association of CSF leukocytes, chemokine, and cytokine responses with 18-week survival.
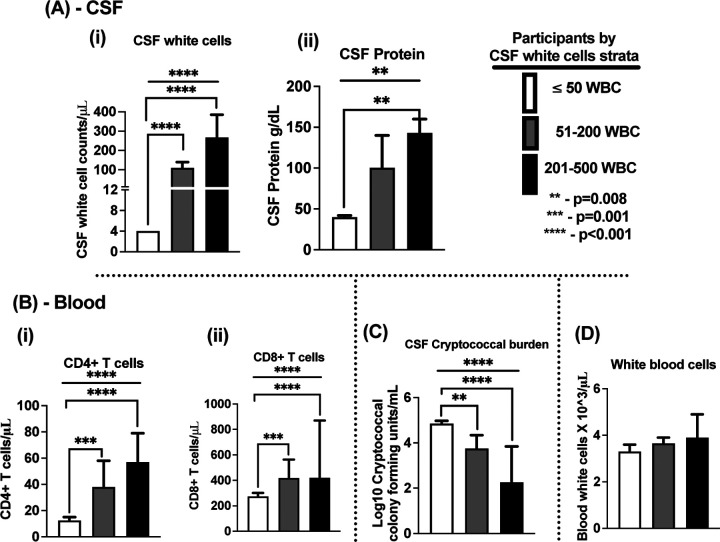
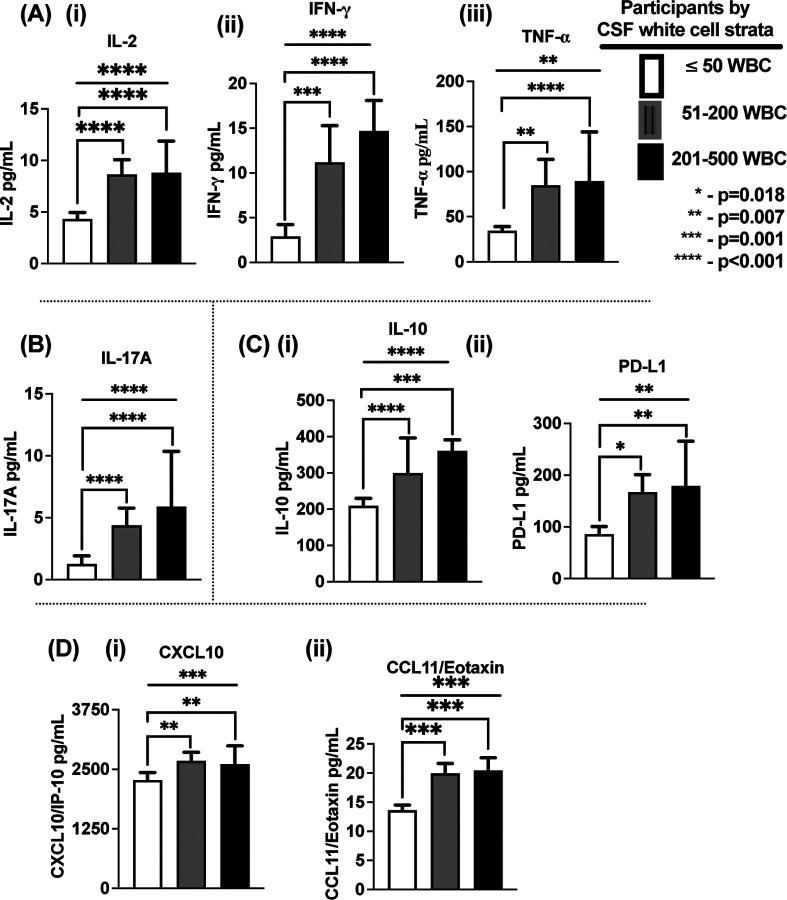
Results: Participants with CSF leukocytes ≥50/μL, had higher probability 68% (52/77) of 18-week survival compared with 52% (151/292) 18-week survival in those with ≤50 cells/μL (Hazard Ratio=1.63, 95% confidence intervals 1.14-2.23; p=0.008). Survival was also associated with higher expression of T helper (Th)-1, Th17 cytokines, and immune regulatory elements. CSF levels of Programmed Death-1 Ligand, CXCL10, and Interleukin (IL)-2 independently predicted survival. In multivariate analysis, CSF leukocytes were inversely associated with CSF fungal burden and positively associated with CSF protein, interferon-gamma (IFN-γ), IL-17A, tumor necrosis factor (TNF)-α, and peripheral blood CD4+ and CD8+ T cells expression.
Conclusion: 18-week survival after diagnosis of cryptococcal meningitis was associated with higher CSF leukocytes at baseline with greater T helper 1 (IFN-γ, IL-2 and TNF-α cytokines), T helper 17 (IL-17A cytokine) and CXCR3+ T cell (CXCL10 chemokine) responses. These results highlight the interdependent contribution of soluble and cellular immune responses in predicting survival with HIV-associated cryptococcal meningitis.
Keywords: CSF white cells; HIV-associated cryptococcal meningitis; antifungal therapy; cerebrospinal fluid; chemokines; cytokines; fungal burden; immune response; survival.
Conflict of interest statement
Authors have declared no substantial conflict of interest. Authors with funding support have declared and acknowledged sources of funding. SO - was a Fogarty and GlaxoSmithKline-Trust in Science Africa funded doctoral scholar at Infectious Diseases Institute, Makerere University. Part of the work contributed to the doctoral successful doctoral thesis examination at the Department of Medical Microbiology, School of Biomedical Sciences, College of Health Sciences, Makerere University [42]. AMK - was a member of a data safety monitoring board.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials