

This is a preprint.
Artificial Intelligence Enabled Prediction of Heart Failure Risk from Single-lead Electrocardiograms
- PMID: 38854022
- PMCID: PMC11160804
- DOI: 10.1101/2024.05.27.24307952
Artificial Intelligence Enabled Prediction of Heart Failure Risk from Single-lead Electrocardiograms
Update in
-
Artificial Intelligence-Enabled Prediction of Heart Failure Risk From Single-Lead Electrocardiograms.JAMA Cardiol. 2025 Jun 1;10(6):574-584. doi: 10.1001/jamacardio.2025.0492. JAMA Cardiol. 2025. PMID: 40238120
Abstract
Importance: Despite the availability of disease-modifying therapies, scalable strategies for heart failure (HF) risk stratification remain elusive. Portable devices capable of recording single-lead electrocardiograms (ECGs) can enable large-scale community-based risk assessment.
Objective: To evaluate an artificial intelligence (AI) algorithm to predict HF risk from noisy single-lead ECGs.
Design: Multicohort study.
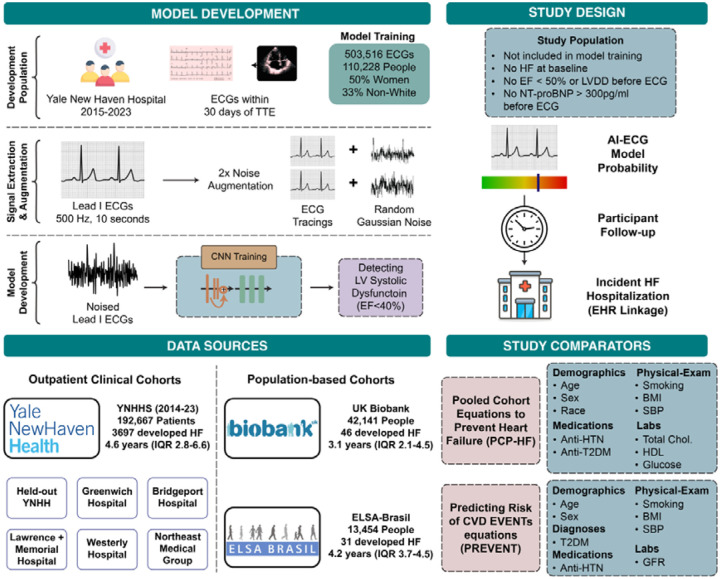
Setting: Retrospective cohort of individuals with outpatient ECGs in the integrated Yale New Haven Health System (YNHHS) and prospective population-based cohorts of UK Biobank (UKB) and Brazilian Longitudinal Study of Adult Health (ELSA-Brasil).
Participants: Individuals without HF at baseline.
Exposures: AI-ECG-defined risk of left ventricular systolic dysfunction (LVSD).
Main outcomes and measures: Among individuals with ECGs, we isolated lead I ECGs and deployed a noise-adapted AI-ECG model trained to identify LVSD. We evaluated the association of the model probability with new-onset HF, defined as the first HF hospitalization. We compared the discrimination of AI-ECG against two risk scores for new-onset HF (PCP-HF and PREVENT equations) using Harrel's C-statistic, integrated discrimination improvement (IDI), and net reclassification improvement (NRI).
Results: There were 192,667 YNHHS patients (age 56 years [IQR, 41-69], 112,082 women [58%]), 42,141 UKB participants (65 years [59-71], 21,795 women [52%]), and 13,454 ELSA-Brasil participants (56 years [41-69], 7,348 women [55%]) with baseline ECGs. A total of 3,697 developed HF in YNHHS over 4.6 years (2.8-6.6), 46 in UKB over 3.1 years (2.1-4.5), and 31 in ELSA-Brasil over 4.2 years (3.7-4.5). A positive AI-ECG screen was associated with a 3- to 7-fold higher risk for HF, and each 0.1 increment in the model probability portended a 27-65% higher hazard across cohorts, independent of age, sex, comorbidities, and competing risk of death. AI-ECG's discrimination for new-onset HF was 0.725 in YNHHS, 0.792 in UKB, and 0.833 in ELSA-Brasil. Across cohorts, incorporating AI-ECG predictions in addition to PCP-HF and PREVENT equations resulted in improved Harrel's C-statistic (ΔPCP-HF=0.112-0.114; ΔPREVENT=0.080-0.101). AI-ECG had IDI of 0.094-0.238 and 0.090-0.192, and NRI of 15.8%-48.8% and 12.8%-36.3%, vs. PCP-HF and PREVENT, respectively.
Conclusions and relevance: Across multinational cohorts, a noise-adapted AI model defined HF risk using lead I ECGs, suggesting a potential portable and wearable device-based HF risk-stratification strategy.
Keywords: Deep learning; Electrocardiograms; Heart failure; Predictive Modelling; Risk Stratification; Wearable Devices.
Conflict of interest statement
Dr. Khera is an Associate Editor of JAMA. Dr. Khera and Mr. Sangha are the coinventors of U.S. Provisional Patent Application No. 63/346,610, “Articles and methods for format-independent detection of hidden cardiovascular disease from printed electrocardiographic images using deep learning” and are co-founders of Ensight-AI. Dr. Khera receives support the National Institutes of Health (under awards R01AG089981, R01HL167858, and K23HL153775) and the Doris Duke Charitable Foundation (under award 2022060). He receives support from the Blavatnik Foundation through the Blavatnik Fund for Innovation at Yale. He also receives research support, through Yale, from Bristol-Myers Squibb, BridgeBio, and Novo Nordisk. In addition to 63/346,610, Dr. Khera is a coinventor of U.S. Pending Patent Applications WO2023230345A1, US20220336048A1, 63/484,426, 63/508,315, 63/580,137, 63/606,203, 63/619,241, and 63/562,335. Dr. Khera and Dr. Oikonomou are co-founders of Evidence2Health, a precision health platform to improve evidence-based cardiovascular care. Dr. Oikonomou is a co-inventor of the U.S. Patent Applications 63/508,315 & 63/177,117 and has been a consultant to Caristo Diagnostics Ltd (all outside the current work). Dr. Krumholz works under contract with the Centers for Medicare & Medicaid Services to support quality measurement programs. He is associated with research contracts through Yale University from Janssen, Kenvue, and Pfizer. In the past three years, Dr. Krumholz received options for Element Science and Identifeye and payments from F-Prime for advisory roles. He is a co-founder of and holds equity in Hugo Health, Refactor Health, and Ensight-AI. Dr. Ribeiro is supported in part by the National Council for Scientific and Technological Development - CNPq (grants 465518/2014-1, 310790/2021-2, 409604/2022-4 e 445011/2023-8). Dr. Brant is supported in part by CNPq (307329/2022-4). Dr. Asselbergs is supported by Heart4Data, which received funding from the Dutch Heart Foundation and ZonMw (2021-B015), and UCL Hospitals NIHR Biomedical Research Centre.
Figures
Similar articles
-
Artificial Intelligence-Enabled Prediction of Heart Failure Risk From Single-Lead Electrocardiograms.JAMA Cardiol. 2025 Jun 1;10(6):574-584. doi: 10.1001/jamacardio.2025.0492. JAMA Cardiol. 2025. PMID: 40238120
-
Heart failure risk stratification using artificial intelligence applied to electrocardiogram images: a multinational study.Eur Heart J. 2025 Mar 13;46(11):1044-1053. doi: 10.1093/eurheartj/ehae914. Eur Heart J. 2025. PMID: 39804243
-
Scalable Risk Stratification for Heart Failure Using Artificial Intelligence applied to 12-lead Electrocardiographic Images: A Multinational Study.medRxiv [Preprint]. 2024 Apr 3:2024.04.02.24305232. doi: 10.1101/2024.04.02.24305232. medRxiv. 2024. Update in: Eur Heart J. 2025 Mar 13;46(11):1044-1053. doi: 10.1093/eurheartj/ehae914. PMID: 38633808 Free PMC article. Updated. Preprint.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Artificial intelligence for diagnosing exudative age-related macular degeneration.Cochrane Database Syst Rev. 2024 Oct 17;10(10):CD015522. doi: 10.1002/14651858.CD015522.pub2. Cochrane Database Syst Rev. 2024. PMID: 39417312
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous