

Prophylactic Left Atrial Appendage Ligation During Coronary Artery Bypass Graft Surgery Allows Safe Avoidance of Anticoagulation Regardless of Postoperative Atrial Fibrillation
- PMID: 38854212
- PMCID: PMC11157991
- DOI: 10.7759/cureus.59876
Prophylactic Left Atrial Appendage Ligation During Coronary Artery Bypass Graft Surgery Allows Safe Avoidance of Anticoagulation Regardless of Postoperative Atrial Fibrillation
Abstract
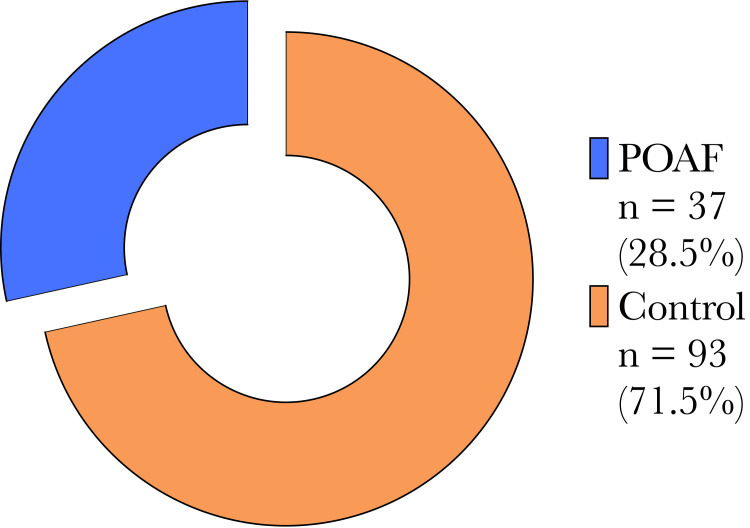
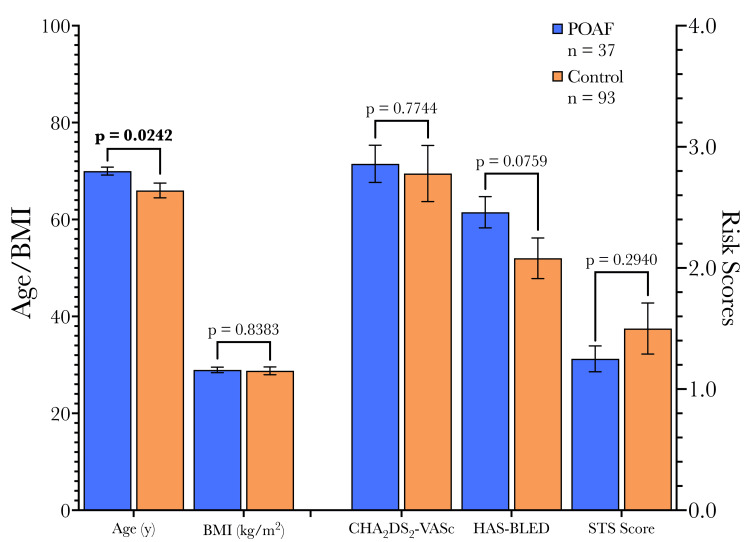
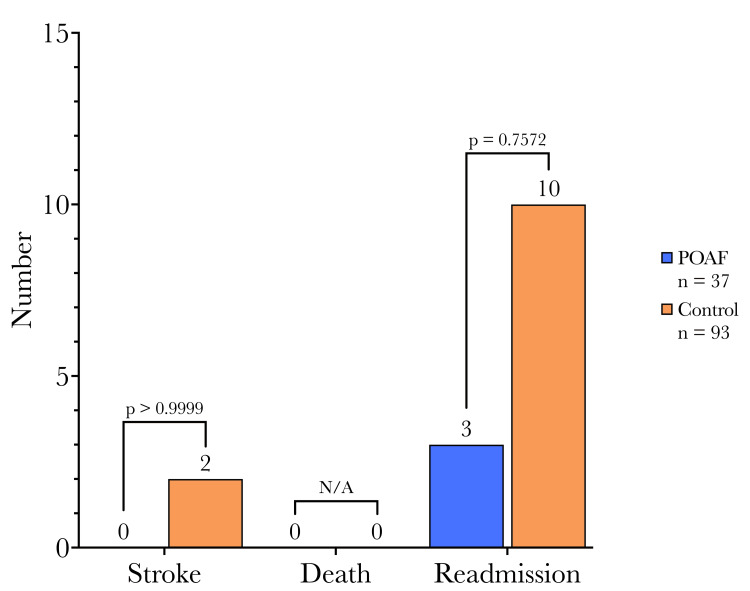
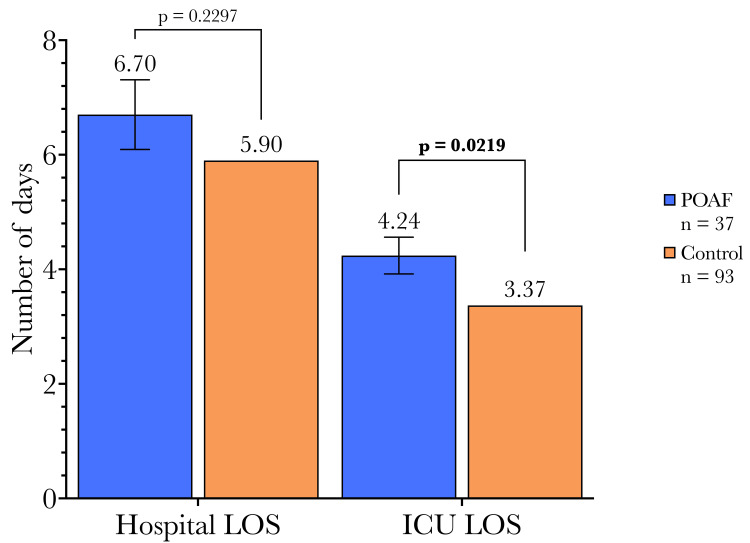
Background New-onset postoperative atrial fibrillation (POAF) is the most common arrhythmia following cardiac surgery. POAF increases the risk of thromboembolism and stroke, as well as morbidity and mortality more generally. Despite evidence from the landmark PROTECT-AF and PREVAIL trials, left atrial appendage ligation (LAAL) is not routinely performed for thromboembolism prophylaxis in POAF, and anticoagulation remains the standard of care along with dual antiplatelet therapy. This study evaluated the efficacy of concomitant LAAL in eliminating the need for postoperative anticoagulation, regardless of POAF development, in patients undergoing coronary artery bypass grafting (CABG). Methods Between 2019 and 2021, 130 patients were selected to undergo concomitant LAAL while undergoing CABG surgery. Patients were then monitored for the incidence of new-onset POAF, and anticoagulation was strictly avoided for this indication. Demographic and outcome data were collected, with endpoints including transient ischemic attack (TIA) or stroke, death, and readmission within one year, as well as the length of hospital and intensive care unit (ICU) admissions. Results POAF occurred in 37 patients (28.5%), consistent with previous reports. However, none of the POAF patients experienced TIA or stroke during the one-year follow-up period, compared to 2 (2.15%) in the non-POAF group, a typical rate of postoperative stroke in such a patient population. No significant differences were observed between POAF and non-POAF cohorts in one-year stroke, all-cause mortality, readmission rates, or total hospital stay. Interestingly, the POAF cohort had a significantly longer mean ICU stay (4.24 vs 3.37 days, p = 0.0219), possibly due to the time required for arrhythmia control before discharge. The study population had a high mean CHA2DS2-VASc score (2.81), indicating an increased risk of thromboembolism, and a high mean HAS-BLED score, suggesting an elevated bleeding risk with anticoagulation. Conclusions LAAL appears to be an effective adjunct to CABG for thromboembolism prophylaxis in POAF. Formal anticoagulation was avoided in this study, with no significant differences in adverse events between POAF and non-POAF groups, suggesting that LAAL may be a suitable alternative to anticoagulation, especially in high-risk patients (e.g., those with elevated CHA2DS2-VASc or HAS-BLED scores). The safety and efficacy of this approach should be corroborated by larger randomized studies, such as the ongoing LeAAPS trial. LAAL during CABG may help reduce the risk of bleeding complications associated with anticoagulation while maintaining protection against thromboembolic events in patients who develop POAF.
Keywords: anticoagulation; coronary artery bypass grafting; left atrial appendage ligation; postoperative atrial fibrillation; stroke.
Copyright © 2024, Khalpey et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Prophylactic left atrial appendage ligation during coronary artery bypass grafting: A propensity score-matched analysis.J Thorac Cardiovasc Surg. 2025 Jul;170(1):207-215. doi: 10.1016/j.jtcvs.2024.08.004. Epub 2024 Aug 15. J Thorac Cardiovasc Surg. 2025. PMID: 39153715
-
Long-term Thromboembolic Risk in Patients With Postoperative Atrial Fibrillation After Coronary Artery Bypass Graft Surgery and Patients With Nonvalvular Atrial Fibrillation.JAMA Cardiol. 2018 May 1;3(5):417-424. doi: 10.1001/jamacardio.2018.0405. JAMA Cardiol. 2018. PMID: 29590304 Free PMC article.
-
Novel Oral Anticoagulants Compared to Warfarin for Postoperative Atrial Fibrillation After Isolated Coronary Artery Bypass Grafting.Heart Lung Circ. 2020 Dec;29(12):1832-1838. doi: 10.1016/j.hlc.2020.04.018. Epub 2020 Jun 14. Heart Lung Circ. 2020. PMID: 32622911
-
Anticoagulation for post-operative atrial fibrillation after isolated coronary artery bypass grafting: a meta-analysis.Eur Heart J. 2024 Aug 3;45(29):2620-2630. doi: 10.1093/eurheartj/ehae267. Eur Heart J. 2024. PMID: 38809189
-
The Management of Postoperative Atrial Fibrillation (POAF): A Systematic Review.Cureus. 2023 Aug 3;15(8):e42880. doi: 10.7759/cureus.42880. eCollection 2023 Aug. Cureus. 2023. PMID: 37664333 Free PMC article. Review.
Cited by
-
Epicardial placement of human placental membrane allografts in coronary artery bypass graft surgery is associated with reduced postoperative atrial fibrillation: a pilot study for a future multi-center randomized controlled trial.J Cardiothorac Surg. 2024 Jun 1;19(1):315. doi: 10.1186/s13019-024-02822-8. J Cardiothorac Surg. 2024. PMID: 38824517 Free PMC article.
-
Surgical Explantation of an Amplatzer Device for Patent Foramen Ovale Closure in a Patient With Nickel Allergy: A Case Report.Clin Case Rep. 2024 Dec 15;12(12):e70006. doi: 10.1002/ccr3.70006. eCollection 2024 Dec. Clin Case Rep. 2024. PMID: 39687653 Free PMC article.
References
-
- Changes in P-wave dispersion and P-wave duration after open heart surgery are associated with the peak incidence of atrial fibrillation. Tsikouris JP, Kluger J, Song J, White CM. Heart Lung. 2001;30:466–471. - PubMed
-
- A perspective of postoperative atrial fibrillation in cardiac operations. Cox JL. Ann Thorac Surg. 1993;56:405–409. - PubMed
LinkOut - more resources
Full Text Sources