

Surgical Orthodontic Treatment for Skeletal Maxillary Protrusion in Sturge-Weber Syndrome: A Case Report and Review of the Literature
- PMID: 38854229
- PMCID: PMC11162147
- DOI: 10.7759/cureus.59964
Surgical Orthodontic Treatment for Skeletal Maxillary Protrusion in Sturge-Weber Syndrome: A Case Report and Review of the Literature
Abstract
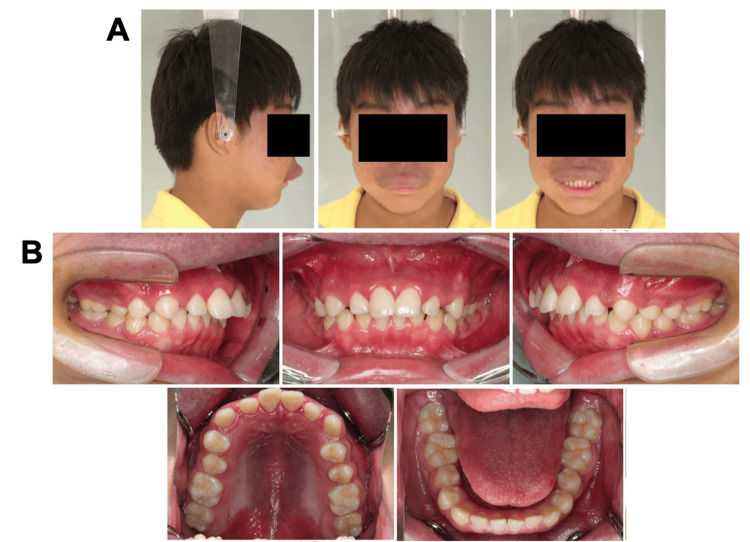
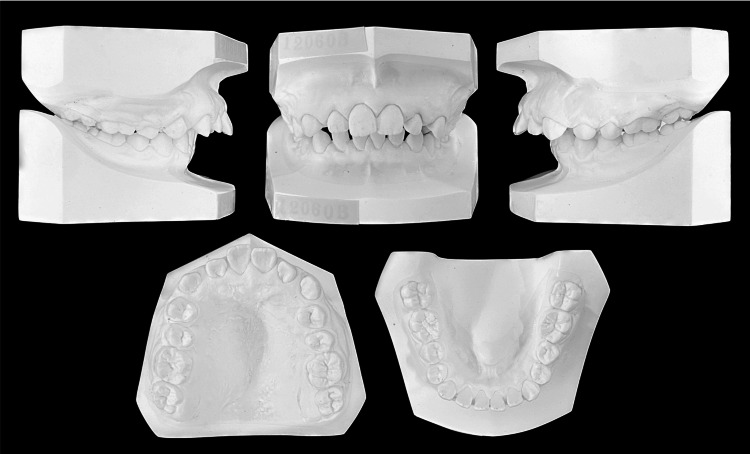
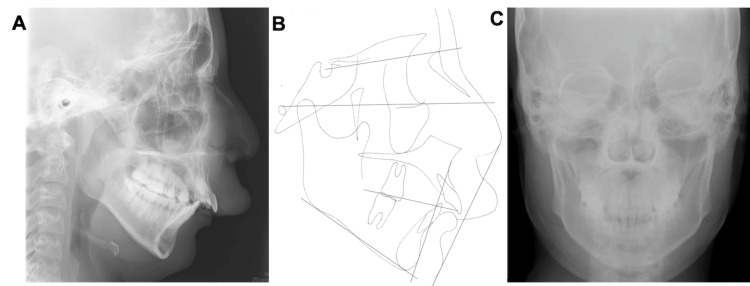
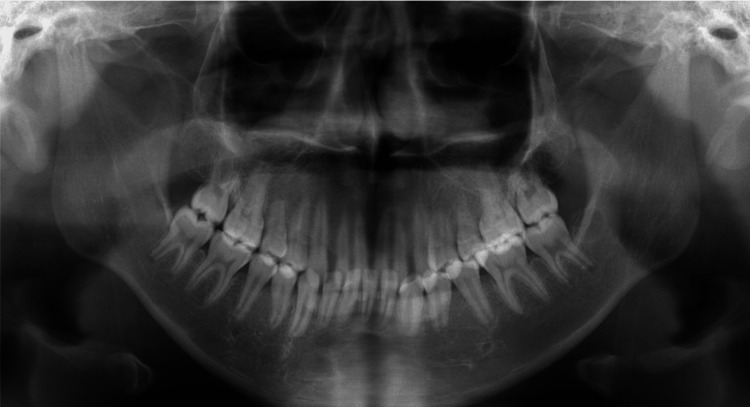
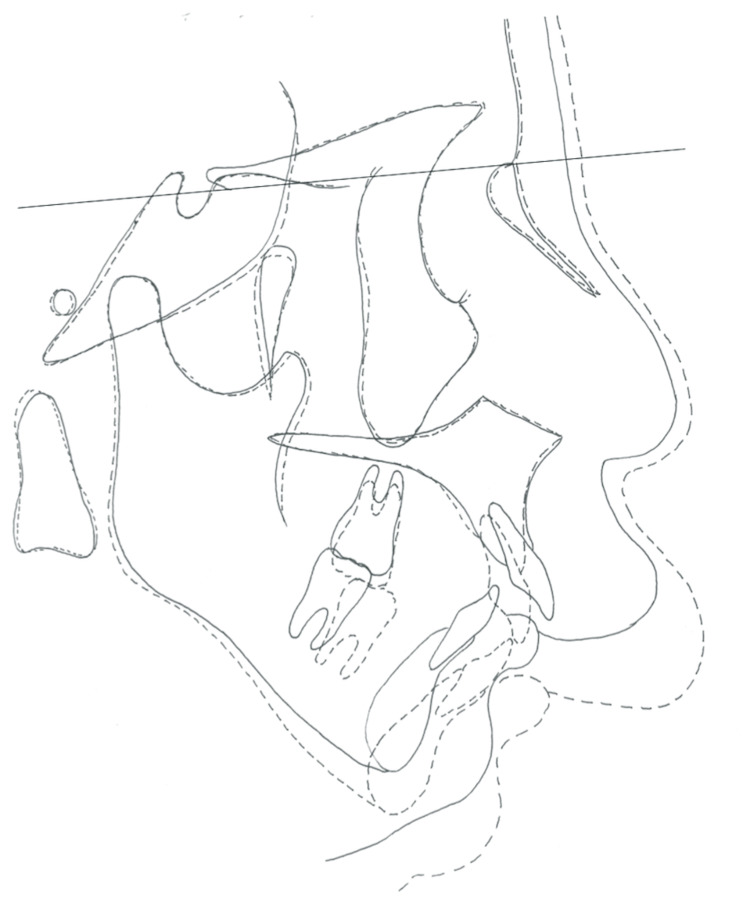
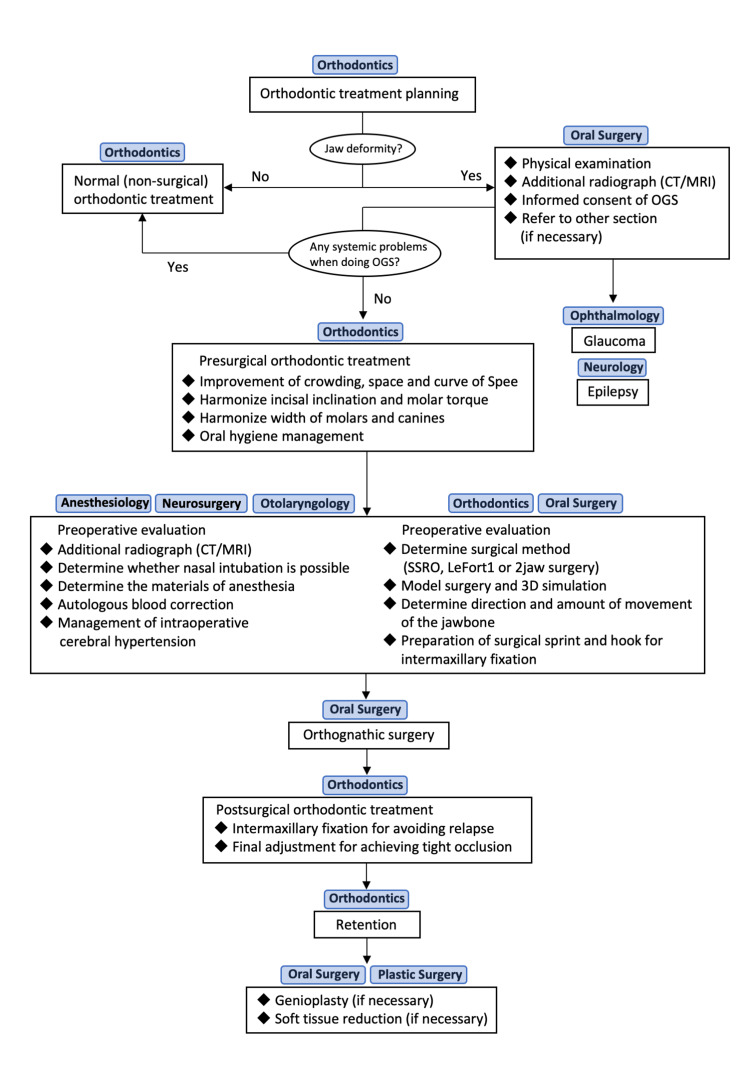
Sturge-Weber syndrome (SWS) is characterized by hemangiomas, glaucoma, and central nervous system disorders. Here, we report the case of a 15-year-old boy with SWS and upper-lip hypertrophy who underwent surgical orthodontic treatment for correction of a large overjet and deep overbite. In addition to the a large overjet and deep overbite, interdental spacing was observed in both the arches. The mandible was retrognathic and deviated to the right side. No maxillary occlusal canting or temporomandibular joint symptoms were observed. The patient was diagnosed with skeletal maxillary protrusion with spaced dentition and mandibular deviation to the right due to SWS. After presurgical orthodontic treatment using a multibracket appliance, we performed a sagittal split ramus osteotomy (SSRO) alone due to the presence of a hemangioma around the maxilla. No abnormal bleeding or cerebral hemorrhage due to increased blood pressure was observed during the SSRO. Postoperatively, the maxillary and mandibular arches were well-aligned, the deep overbite and excessive overjet improved, and bilateral angle class I molar and canine relationships were established. Furthermore, mandibular deviation improved, and the midlines of both arches approximately coincided with the facial midline. In conclusion, orthognathic surgery is feasible in patients with SWS after carefully evaluating the sites and sizes of the hemangiomas.
Keywords: hemangioma; orthodontic treatment; sagittal split ramus osteotomy; skeletal maxillary protrusion; sturge-weber syndrome.
Copyright © 2024, Kado et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Surgical Orthodontic Treatment Involving Mandibular Premolar Extraction in Patient with Mandibular Retrusion Associated with Temporomandibular Joint Osteoarthritis.Bull Tokyo Dent Coll. 2019 Jun 21;60(2):139-149. doi: 10.2209/tdcpublication.2018-0047. Epub 2019 Apr 10. Bull Tokyo Dent Coll. 2019. PMID: 30971679
-
Nonsurgical maxillary orthopedic protraction treatment for an adult patient with hyperdivergent facial morphology, Class III malocclusion, and bilateral crossbite.Am J Orthod Dentofacial Orthop. 2022 Aug;162(2):264-278. doi: 10.1016/j.ajodo.2021.02.027. Epub 2022 May 6. Am J Orthod Dentofacial Orthop. 2022. PMID: 35534400
-
Severe Class II malocclusion with facial asymmetry treated with intraoral vertico-sagittal ramus osteotomy and LeFort I osteotomy.Am J Orthod Dentofacial Orthop. 2009 Jun;135(6):809-19. doi: 10.1016/j.ajodo.2006.11.026. Am J Orthod Dentofacial Orthop. 2009. PMID: 19524842
-
Multidisciplinary treatment with a customized lingual appliance for an adult patient with severe Class III malocclusion and multiple missing teeth.Am J Orthod Dentofacial Orthop. 2019 Sep;156(3):401-411. doi: 10.1016/j.ajodo.2019.05.004. Am J Orthod Dentofacial Orthop. 2019. PMID: 31474270
-
Substantial Improvements in Facial Morphology through Surgical-Orthodontic Treatment: A Case Report and Literature Review.Medicina (Kaunas). 2022 Aug 3;58(8):1043. doi: 10.3390/medicina58081043. Medicina (Kaunas). 2022. PMID: 36013510 Free PMC article. Review.
References
-
- Analysis of Sturge-Weber syndrome: a retrospective study of multiple associated variables. Maraña Pérez AI, Ruiz-Falcó Rojas ML, Puertas Martín V, Domínguez Carral J, Carreras Sáez I, Duat Rodríguez A, Sánchez González V. Neurologia. 2017;32:363–370. - PubMed
-
- Neurocutaneous syndromes. Roach ES. Pediatr Clin North Am. 1992;39:591–620. - PubMed
Publication types
LinkOut - more resources
Full Text Sources