

Strain Differences in Bloodstream and Skin Infection: Methicillin-Resistant Staphylococcus aureus Isolated in 2018-2021 in a Single Health System
- PMID: 38854395
- PMCID: PMC11160326
- DOI: 10.1093/ofid/ofae261
Strain Differences in Bloodstream and Skin Infection: Methicillin-Resistant Staphylococcus aureus Isolated in 2018-2021 in a Single Health System
Abstract
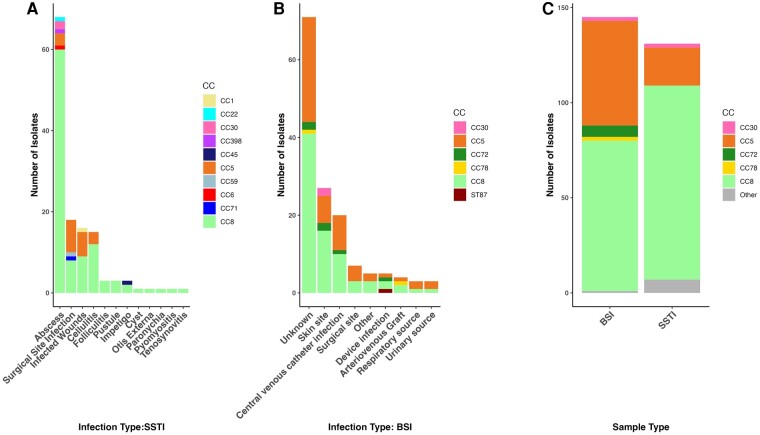
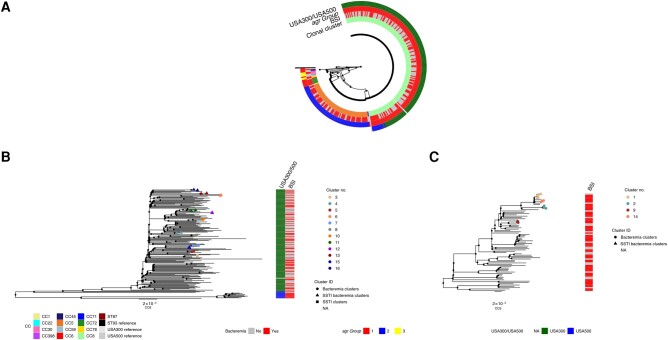
Staphylococcus aureus is a common cause of skin and soft-tissue infections (SSTIs) and has become the most common cause of bloodstream infections (BSIs) in recent years, but whether the strains causing these two clinical syndromes overlap has not been studied adequately. USA300/500 (clonal complex [CC] 8-sequence type [ST] 8) and USA100 (CC5-ST5) have dominated among methicillin-resistant S aureus (MRSA) strains in the United States since the early 2000s. We compared the genomes of unselected MRSA isolates from 131 SSTIs with those from 145 BSIs at a single US center in overlapping periods in 2018-2021. CC8 MRSA was more common among SSTIs, and CC5 was more common among BSIs, consistent with prior literature. Based on clustering genomes with a threshold of 15 single-nucleotide polymorphisms, we identified clusters limited to patients with SSTI and separate clusters exclusively comprising patients with BSIs. However, we also identified eight clusters that included at least one SSTI and one BSI isolate. This suggests that virulent MRSA strains are transmitted from person to person locally in the healthcare setting or the community and that single lineages are often capable of causing both SSTIs and BSIs.
Keywords: CC5; CC8; Staphylococcus aureus; clonal complex; whole-genome sequencing.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. M. Z. D. reports support from GSK and Covance for clinical trials; service on a GSK advisor board; a contract from Johnson & Johnson to prepare a research report; and an honorarium for a lecture at the University of Iowa. All other authors report no potential conflicts.
Figures
References
-
- Wertheim HF, Vos MC, Ott A, et al. Risk and outcome of nosocomial Staphylococcus aureus bacteraemia in nasal carriers versus non-carriers. Lancet 2004; 364:703–5. - PubMed
